

Non-retroareolar male mucinous breast cancer without gynecomastia development in an elderly man: A case report
- PMID: 37727495
- PMCID: PMC10506025
- DOI: 10.12998/wjcc.v11.i25.5954
Non-retroareolar male mucinous breast cancer without gynecomastia development in an elderly man: A case report
Abstract
Background: Male breast cancer (MBC) is an extremely rare condition and accounts for less than 1% of all breast cancers, and malignant tumors occur in less than 1% of the affected men. Mucinous breast cancer is extremely rare and accounts for 2% of all invasive breast cancers. Generally, MBC is accompanied by a retroareolar mass.
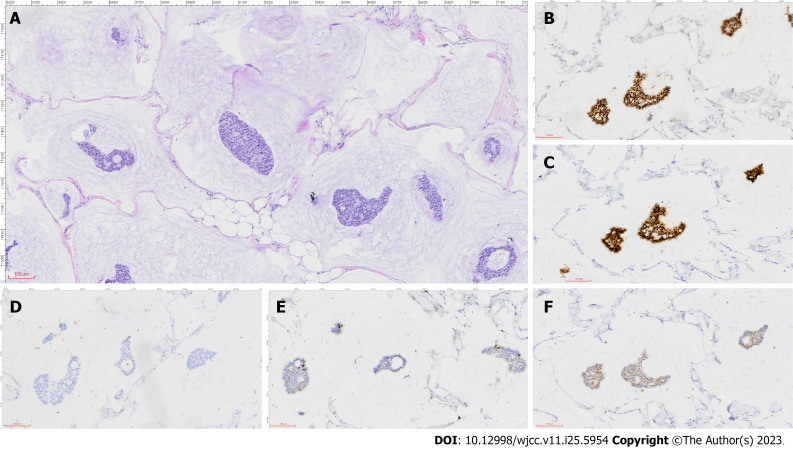
Case summary: Herein, we report a case of male mucinous breast carcinoma (MMBC) without gynecomastia development and with mass localization outside the common retroareolar region, wherein the mass was a painless nodule in the right breast of a 64-year-old man. We also discuss the clinical and pathological characteristics of this unusual tumor. The excised breast specimen showed pure mucinous carcinoma. The patient had strong expression of estrogen and progesterone receptors, a low Ki-67 proliferation index of the tumor cells, and negative pathological axillary lymph nodes. The patient underwent modified radical mastectomy and axillary lymph node dissection, followed by tamoxifen hormone therapy.
Conclusion: To the best of our knowledge, this is the first case report of MMBC in the non-retroareolar region of the nipple without gynecomastia development. Mucinous tumors are easily missed during diagnosis, and the incidence of axillary lymph node metastases of chest mucinous tumors has increased.
Keywords: Breast cancer; Case report; Male; Mucinous adenocarcinoma; Nipple.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures


Similar articles
-
Mucinous carcinoma with axillary lymph node metastasis in a male breast: A case report.N Am J Med Sci. 2010 Feb;2(2):111-3. N Am J Med Sci. 2010. PMID: 22624124 Free PMC article.
-
Pure mucinous carcinoma with axillary lymph node metastasis in a male breast.Breast Cancer. 2012 Oct;19(4):365-8. doi: 10.1007/s12282-009-0163-3. Epub 2009 Sep 10. Breast Cancer. 2012. PMID: 19756925
-
Isoechoic axillary lymph node metastases of mucinous carcinoma of the breast: a case report.Breast Cancer. 2006;13(4):382-5. doi: 10.2325/jbcs.13.382. Breast Cancer. 2006. PMID: 17146168
-
Strategies in treating male breast cancer.Expert Opin Pharmacother. 2007 Feb;8(2):193-202. doi: 10.1517/14656566.8.2.193. Expert Opin Pharmacother. 2007. PMID: 17257089 Review.
-
Ataxia Telangiectasia in a Patient with Breast Cancer: A Case Report.Tokai J Exp Clin Med. 2023 Sep 20;48(3):95-98. Tokai J Exp Clin Med. 2023. PMID: 37635070 Review.
References
-
- Fox S, Speirs V, Shaaban AM. Male breast cancer: an update. Virchows Arch. 2022;480:85–93. - PubMed
-
- Limaiem F, Ahmad F. Mucinous Breast Carcinoma. 2023 Feb 12. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan- - PubMed
-
- Fentiman IS, Fourquet A, Hortobagyi GN. Male breast cancer. Lancet. 2006;367:595–604. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
