

Experience With Adaptive Servo-Ventilation Among Veterans in the Post-SERVE-HF Era
- PMID: 37727510
- PMCID: PMC10506493
- DOI: 10.12788/fp.0374
Experience With Adaptive Servo-Ventilation Among Veterans in the Post-SERVE-HF Era
Abstract
Background: The sleep medicine community has struggled to identify the ideal role for adaptive servo-ventilation (ASV) therapy following a study that found increased mortality in patients with central sleep apnea (CSA) and heart failure with reduced ejection fraction who used ASV therapy. We aimed to identify characteristics of patients who benefit from ASV therapy.
Methods: We performed a record review of all patients treated with ASV therapy at the Hampton Veterans Affairs Medical Center in Virginia from January 1, 2015, to April 30, 2020. Clinical and polysomnographic characteristics of patients adherent to therapy were compared with those that were not adherent.
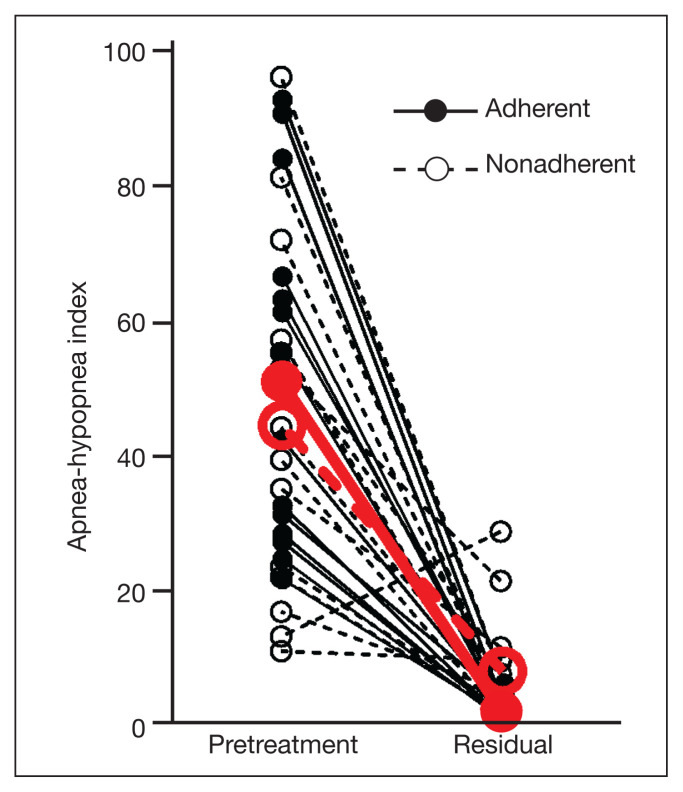
Results: Our cohort of 31 patients was entirely male with a mean age of 67.2 years, body mass index of 34.0, and Epworth Sleepiness Scale score of 10.9. Primary CSA was initially diagnosed in 3 patients (10%), comorbid obstructive sleep apnea (OSA) and CSA in 9 (29%), and primary OSA in 19 (61%). Seventeen patients (55%) met minimal adherence criteria with ASV therapy. The obstructive apnea-hypopnea index (AHI), as a proportion of the total pretreatment AHI, was higher in adherent patients (81.5%) vs nonadherent patients (46.7%) (P = .02). The median residual AHI was lower in the adherent group, both as absolute values (1.7 vs 4.7 events/h; P = .004) and as a percentage of the pretreatment AHI (3.1% vs 10.2%; P = .002).
Conclusions: Patients using ASV devices regularly have a larger component of obstructive sleep-disordered breathing and obtain greater objective benefit from ASV than those that do not. This understanding may help to identify patients that will most benefit from this debated form of therapy.
Copyright © 2023 Frontline Medical Communications Inc., Parsippany, NJ, USA.
Conflict of interest statement
Author disclosures The authors report no actual or potential conflicts of interest or outside sources of funding with regard to this article.
Figures

Similar articles
-
Adaptive servo-ventilation for sleep-disordered breathing in patients with heart failure with reduced ejection fraction (ADVENT-HF): a multicentre, multinational, parallel-group, open-label, phase 3 randomised controlled trial.Lancet Respir Med. 2024 Feb;12(2):153-166. doi: 10.1016/S2213-2600(23)00374-0. Epub 2023 Dec 21. Lancet Respir Med. 2024. PMID: 38142697 Clinical Trial.
-
What is the remaining status of adaptive servo-ventilation? The results of a real-life multicenter study (OTRLASV-study) : Adaptive servo-ventilation in real-life conditions.Respir Res. 2019 Oct 29;20(1):235. doi: 10.1186/s12931-019-1221-9. Respir Res. 2019. PMID: 31665026 Free PMC article. Clinical Trial.
-
Patterns of adaptive servo-ventilation settings in a real-life multicenter study: pay attention to volume! : Adaptive servo-ventilation settings in real-life conditions.Respir Res. 2020 Sep 21;21(1):243. doi: 10.1186/s12931-020-01509-7. Respir Res. 2020. PMID: 32957983 Free PMC article. Clinical Trial.
-
Servo-Ventilation Therapy for Sleep-Disordered Breathing.Chest. 2018 Jun;153(6):1501-1502. doi: 10.1016/j.chest.2018.03.052. Chest. 2018. PMID: 29884256 Review.
-
Use of adaptive servo ventilation therapy as treatment of sleep-disordered breathing and heart failure: a systematic review and meta-analysis.Sleep Breath. 2020 Mar;24(1):49-63. doi: 10.1007/s11325-019-01882-8. Epub 2019 Jul 3. Sleep Breath. 2020. PMID: 31270726
References
-
- Verbraecken J. Complex sleep apnoea syndrome. Breathe. 2013;9(5):372–380. doi: 10.1183/20734735.042412. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous