

Role of Dermoscopy in Laser Therapy
- PMID: 37727557
- PMCID: PMC10506824
- DOI: 10.4103/idoj.idoj_325_22
Role of Dermoscopy in Laser Therapy
Abstract
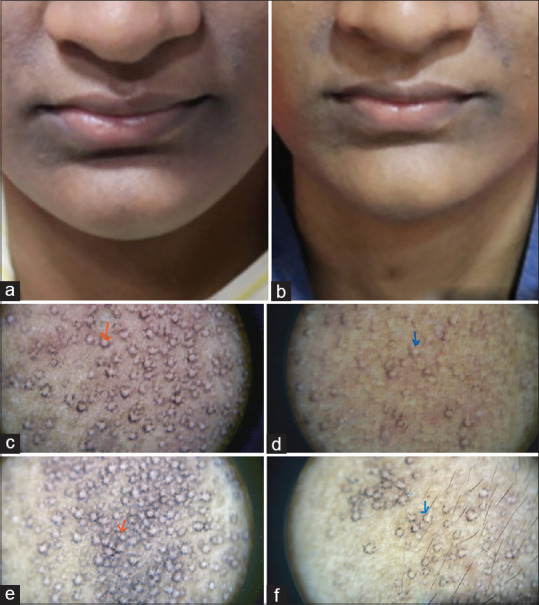
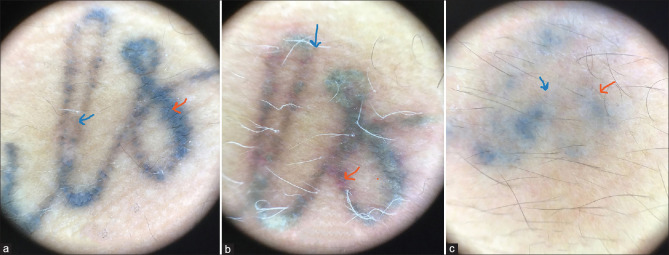
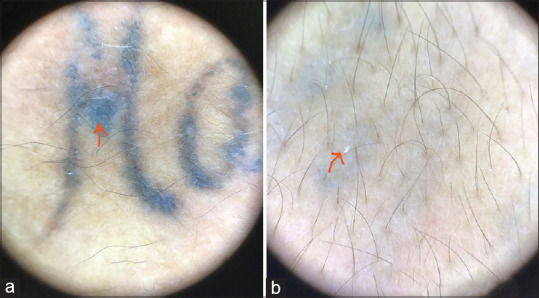
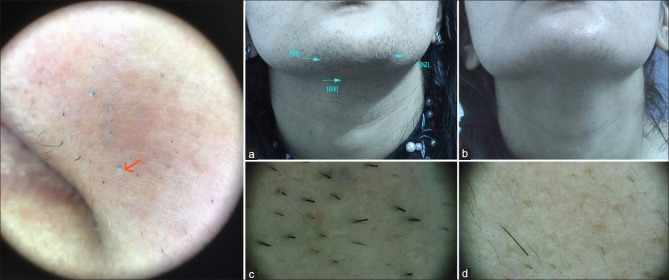
Lasers have revolutionized the interventional dermatology field over the last two decades. Dermatologic conditions previously untreatable are now treated with lasers and lights. A large number of laser systems with advances in technologies have expanded applications of lasers for conditions like birth marks, acne scars, wrinkles, pigmentation, etc. Newer avenues and protocols are now set to treat skin conditions with lasers. The applicability of laser for any indication is dependent on laser tissue interaction which is well documented. For a successful outcome with laser therapy, a right end point of treatment should be achieved. The laser physician often adjusts parameters for laser therapy depending on tissue response, the ultimate aim being achieving optimum outcome with minimum side effects. Gadget based skin evaluation techniques are now an integral part of dermatology and are extending to interventional dermatology too. Application of dermoscopy before, during, and after lasers in various indications has been documented and reviewed. The representative cases highlighted in article emphasize the added dimension to non-invasive diagnostic capabilities of a dermatologist by enabling subsurface microscopy and enhancing therapy outcomes, and incorporation of these into daily practice offers value addition to not only evaluation but also gauging response to therapies. Use of dermoscopy before, during, and after laser therapies is an invaluable non-invasive tool to assess the right indication, initiate appropriate priming, achieve good end point, gauge untoward side effects, achieve good results, and engage patient confidentiality. Comparison of high magnification digital images is also enabled by digital videodermoscopy. Structured studies and protocols are needed to standardize the use of dermoscopy integrated with laser procedures.
Keywords: Dermoscopy; end point; lasers; tissue interaction.
Copyright: © 2023 Indian Dermatology Online Journal.
Conflict of interest statement
There are no conflicts of interest.
Figures

Similar articles
-
Fractional lasers in dermatology--current status and recommendations.Indian J Dermatol Venereol Leprol. 2011 May-Jun;77(3):369-79. doi: 10.4103/0378-6323.79732. Indian J Dermatol Venereol Leprol. 2011. PMID: 21508586
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
-
Lasers and laser-like devices: part one.Australas J Dermatol. 2013 Aug;54(3):173-83. doi: 10.1111/ajd.12034. Epub 2013 Apr 10. Australas J Dermatol. 2013. PMID: 23573909 Review.
-
Vascular lasers and IPLS: guidelines for care from the European Society for Laser Dermatology (ESLD).J Cosmet Laser Ther. 2007 Jun;9(2):113-24. doi: 10.1080/14764170701280693. J Cosmet Laser Ther. 2007. PMID: 17558762 Review.
-
Standard guidelines of care: CO2 laser for removal of benign skin lesions and resurfacing.Indian J Dermatol Venereol Leprol. 2008 Jan;74 Suppl:S61-7. Indian J Dermatol Venereol Leprol. 2008. PMID: 18688106
Cited by
-
Effective Treatment of Rosacea and Other Vascular Lesions Using Intense Pulsed Light System Emitting Vascular Chromophore-Specific Wavelengths: A Clinical and Dermoscopical Analysis.J Clin Med. 2024 Mar 13;13(6):1646. doi: 10.3390/jcm13061646. J Clin Med. 2024. PMID: 38541871 Free PMC article.
References
-
- Cheng CY. Intratherapeutic dermoscopy assists nevus removal by laser therapy. Indian J Dermatol Venereol Leprol. 2020;86:604–5. - PubMed
-
- FotoFinder Systems, Inc. [[Last accessed on 2017 Dec 17]]. Available from: http://www.fotofinder-systems.com/company/about-us/
-
- Hibler BP, Qi Q, Rossi AM. Current state of imaging in dermatology. Semin Cutan Med Surg. 2016;35:2–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
