

The burden of antimicrobial resistance in the Americas in 2019: a cross-country systematic analysis
- PMID: 37727594
- PMCID: PMC10505822
- DOI: 10.1016/j.lana.2023.100561
The burden of antimicrobial resistance in the Americas in 2019: a cross-country systematic analysis
Erratum in
-
Correction to "The burden of antimicrobial resistance in the Americas in 2019: a cross-country systematic analysis" The Lancet Regional Health-Americas 2023; 25, 100561.Lancet Reg Health Am. 2023 Nov 10;28:100632. doi: 10.1016/j.lana.2023.100632. eCollection 2023 Dec. Lancet Reg Health Am. 2023. PMID: 38033356 Free PMC article.
Abstract
Background: Antimicrobial resistance (AMR) is an urgent global health challenge and a critical threat to modern health care. Quantifying its burden in the WHO Region of the Americas has been elusive-despite the region's long history of resistance surveillance. This study provides comprehensive estimates of AMR burden in the Americas to assess this growing health threat.
Methods: We estimated deaths and disability-adjusted life-years (DALYs) attributable to and associated with AMR for 23 bacterial pathogens and 88 pathogen-drug combinations for countries in the WHO Region of the Americas in 2019. We obtained data from mortality registries, surveillance systems, hospital systems, systematic literature reviews, and other sources, and applied predictive statistical modelling to produce estimates of AMR burden for all countries in the Americas. Five broad components were the backbone of our approach: the number of deaths where infection had a role, the proportion of infectious deaths attributable to a given infectious syndrome, the proportion of infectious syndrome deaths attributable to a given pathogen, the percentage of pathogens resistant to an antibiotic class, and the excess risk of mortality (or duration of an infection) associated with this resistance. We then used these components to estimate the disease burden by applying two counterfactual scenarios: deaths attributable to AMR (compared to an alternative scenario where resistant infections are replaced with susceptible ones), and deaths associated with AMR (compared to an alternative scenario where resistant infections would not occur at all). We generated 95% uncertainty intervals (UIs) for final estimates as the 25th and 975th ordered values across 1000 posterior draws, and models were cross-validated for out-of-sample predictive validity.
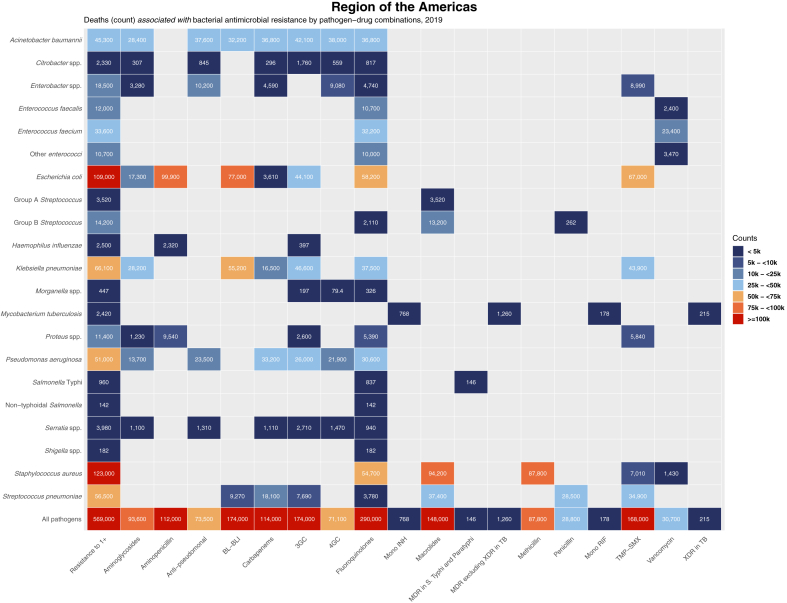
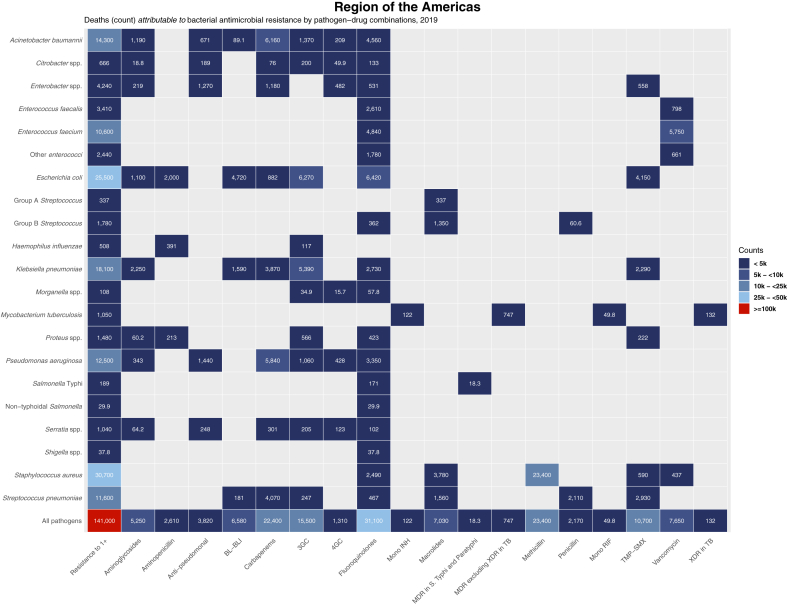
Findings: We estimated 569,000 deaths (95% UI 406,000-771,000) associated with bacterial AMR and 141,000 deaths (99,900-196,000) attributable to bacterial AMR among the 35 countries in the WHO Region of the Americas in 2019. Lower respiratory and thorax infections, as a syndrome, were responsible for the largest fatal burden of AMR in the region, with 189,000 deaths (149,000-241,000) associated with resistance, followed by bloodstream infections (169,000 deaths [94,200-278,000]) and peritoneal/intra-abdominal infections (118,000 deaths [78,600-168,000]). The six leading pathogens (by order of number of deaths associated with resistance) were Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Streptococcus pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii. Together, these pathogens were responsible for 452,000 deaths (326,000-608,000) associated with AMR. Methicillin-resistant S. aureus predominated as the leading pathogen-drug combination in 34 countries for deaths attributable to AMR, while aminopenicillin-resistant E. coli was the leading pathogen-drug combination in 15 countries for deaths associated with AMR.
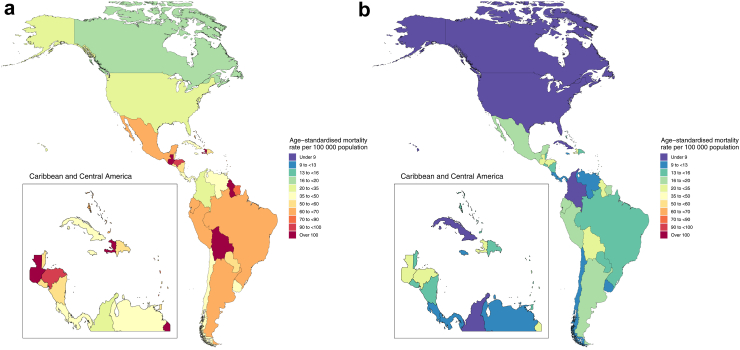
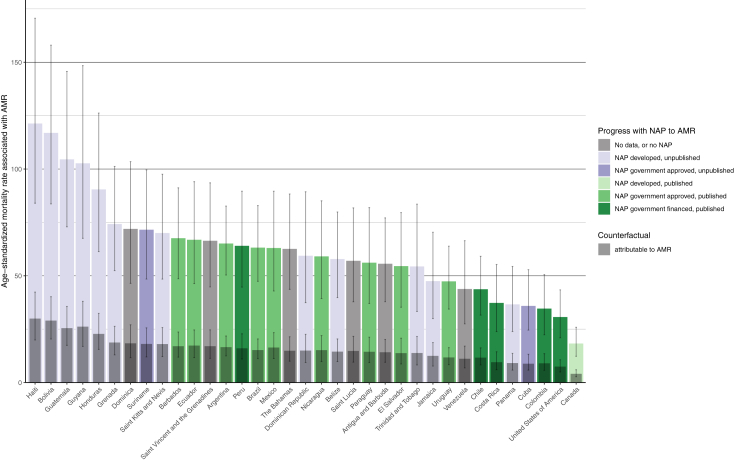
Interpretation: Given the burden across different countries, infectious syndromes, and pathogen-drug combinations, AMR represents a substantial health threat in the Americas. Countries with low access to antibiotics and basic health-care services often face the largest age-standardised mortality rates associated with and attributable to AMR in the region, implicating specific policy interventions. Evidence from this study can guide mitigation efforts that are tailored to the needs of each country in the region while informing decisions regarding funding and resource allocation. Multisectoral and joint cooperative efforts among countries will be a key to success in tackling AMR in the Americas.
Funding: Bill & Melinda Gates Foundation, Wellcome Trust, and Department of Health and Social Care using UK aid funding managed by the Fleming Fund.
Keywords: AMR; Americas; Antimicrobial resistance; Bacteria; Disease burden; Mortality.
© 2023 Published by Elsevier Ltd.
Conflict of interest statement
E Chung reports support for this work in part by the National Institutes of Health (NICHD T32HD007233 to EC). F Krapp reports grants or contracts from the Belgian Directorate of Development Cooperation (DGD) through the Framework Agreement between the Belgian DGD and the Institute of Tropical Medicine, Belgium; the Fogarty International Center of the National Institutes of Health and the University of California Global Health Institute under Award Number D43TW009343; and the Fogarty International Center and National Institute of Child Health & Human Development of the National Institutes of Health under Award Number D43 TW009763; all outside the submitted work. A Pollard reports grants or contracts paid to their institution from The Bill & Melinda Gates Foundation, Wellcome Trust, Coalition for Epidemic Preparedness Innovations (CEPI), Medical Research Council (MRC), and National Institute for Health and Care Research (NIHR); royalties or licenses from AstraZeneca in partnership with Oxford University for development of COVID-19 vaccines; consulting fees from Shionogi; and unpaid leadership or fiduciary roles as Chair of the Department of Health and Social Care’s Joint Committee on Vaccination and Immunisation, and as member of the World Health Organization (WHO) Strategic Advisory Group of Experts on Immunization (SAGE) until 2022; all outside the submitted work. K E Rudd reports support for the present manuscript from National Institutes of Health (NIH) National Heart, Lung, and Blood Institute (NHLBI) (grant T32HL007287) and NIH National Institute of General Medical Sciences (NIGMS) (grant K23GM141463); and reports consulting fees from Janssen Pharmaceuticals outside the submitted work. J Sifuentes-Osornio reports grants or contracts from Roches Pharmaceuticals (protocol number: GA42469) and Novartis Pharmaceuticals (RUXCOVID clinical trial) outside the submitted work.
Figures
References
-
- WHO . 2021. Antimicrobial resistance.https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance
-
- O’Neill J. The Review on Antimicrobial Resistance; London, UK: 2016. Tackling drug-resistant infections globally: final report and recommendations.https://apo.org.au/node/63983
-
- National Office for Animal Health . 2016. NOAH response to final O Neill AMR review report.https://www.noah.co.uk/wp-content/uploads/2016/07/FINAL-NOAH-response-to... Middlesex, UK.
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
