

Contribution of active surveillance cultures to the control of hospital-acquired carbapenem-resistant Acinetobacter baumannii in an endemic hospital setting
- PMID: 37728054
- PMCID: PMC10877541
- DOI: 10.1017/ice.2023.162
Contribution of active surveillance cultures to the control of hospital-acquired carbapenem-resistant Acinetobacter baumannii in an endemic hospital setting
Abstract
Background: Despite the increasing rates of carbapenem-resistant Acinetobacter baumannii (CRAB) carriage among hospitalized patients in endemic settings, the role of active surveillance cultures and cohorting is still debated. We sought to determine the long-term effect of a multifaceted infection-control intervention on the incidence of CRAB in an endemic setting.
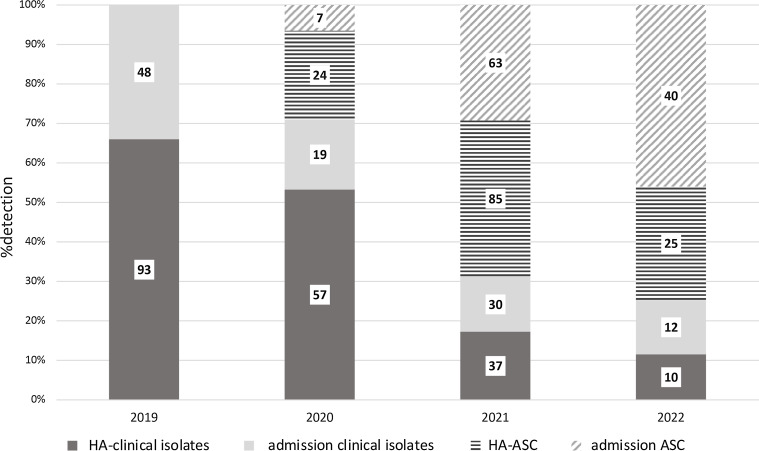
Methods: A prospective, quasi-experimental study was performed at a 670-bed, acute-care hospital. The study consisted of 4 phases. In phase I, basic infection control measures were used. In phase II, CRAB carriers were cohorted in a single ward with dedicated nursing and enhanced environmental cleaning. In phase III large-scale screening in high-risk units was implemented. Phase IV comprised a 15-month follow-up period.
Results: During the baseline period, the mean incidence rate (IDR) of CRAB was 44 per 100,000 patient days (95% CI, 37.7-54.1). No significant decrease was observed during phase II (IDR, 40.8 per 100,000 patient days; 95% CI, 30.0-56.7; P = .97). During phase III, despite high compliance with control measures, ongoing transmission in several wards was observed and the mean IDR was 53.9 per 100,000 patient days (95% CI, 40.5-72.2; P = .55). In phase IV, following the implementation of large-scale screening, a significant decrease in the mean IDR was observed (25.8 per 100,000 patient days; 95% CI, 19.9-33.5; P = .03). An overall reduction of CRAB rate was observed between phase I and phase IV (rate ratio, 0.6; 95% CI, 0.4-0.9; P < .001).
Conclusions: The comprehensive intervention that included intensified control measures with routine active screening cultures was effective in reducing the incidence of CRAB in an endemic hospital setting.
Conflict of interest statement
All authors report no conflicts of interest relevant to this article.
Figures




References
-
- Glew RH, Moellering RCJ, Kunz LJ. Infections with Acinetobacter calcoaceticus (Herellea vaginicola): clinical and laboratory studies. Medicine (Baltimore) 1977;56:79–97. - PubMed
-
- Higgins PG, Dammhayn C, Hackel M, Seifert H. Global spread of carbapenem-resistant Acinetobacter baumannii . J Antimicrob Chemother 2010;65:233–238. - PubMed
-
- Antimicrobial resistance surveillance in Europe 2022–2020 data. European Centers for Disease Prevention and Control website. https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance.... Published 2022. Accessed December 24 2022.
-
- Chung DR, Song JH, Kim SH, et al. High prevalence of multidrug-resistant nonfermenters in hospital-acquired pneumonia in Asia. Am J Respir Crit Care Med 2011;184:1409–1417. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
