

Cost-effectiveness of CT perfusion for the detection of large vessel occlusion acute ischemic stroke followed by endovascular treatment: a model-based health economic evaluation study
- PMID: 37728778
- PMCID: PMC10957700
- DOI: 10.1007/s00330-023-10119-y
Cost-effectiveness of CT perfusion for the detection of large vessel occlusion acute ischemic stroke followed by endovascular treatment: a model-based health economic evaluation study
Abstract
Objectives: CT perfusion (CTP) has been suggested to increase the rate of large vessel occlusion (LVO) detection in patients suspected of acute ischemic stroke (AIS) if used in addition to a standard diagnostic imaging regime of CT angiography (CTA) and non-contrast CT (NCCT). The aim of this study was to estimate the costs and health effects of additional CTP for endovascular treatment (EVT)-eligible occlusion detection using model-based analyses.
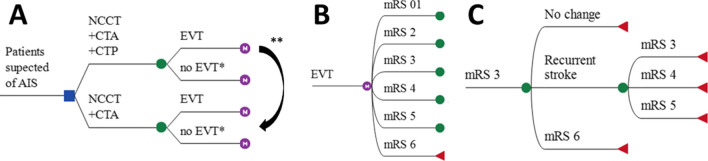
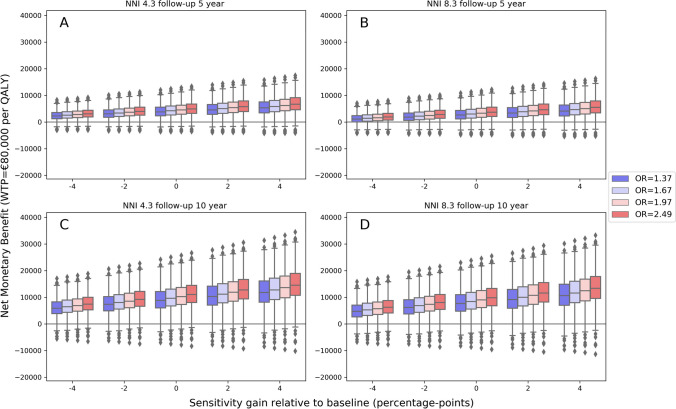
Methods: In this Dutch, nationwide retrospective cohort study with model-based health economic evaluation, data from 701 EVT-treated patients with available CTP results were included (January 2018-March 2022; trialregister.nl:NL7974). We compared a cohort undergoing NCCT, CTA, and CTP (NCCT + CTA + CTP) with a generated counterfactual where NCCT and CTA (NCCT + CTA) was used for LVO detection. The NCCT + CTA strategy was simulated using diagnostic accuracy values and EVT effects from the literature. A Markov model was used to simulate 10-year follow-up. We adopted a healthcare payer perspective for costs in euros and health gains in quality-adjusted life years (QALYs). The primary outcome was the net monetary benefit (NMB) at a willingness to pay of €80,000; secondary outcomes were the difference between LVO detection strategies in QALYs (ΔQALY) and costs (ΔCosts) per LVO patient.
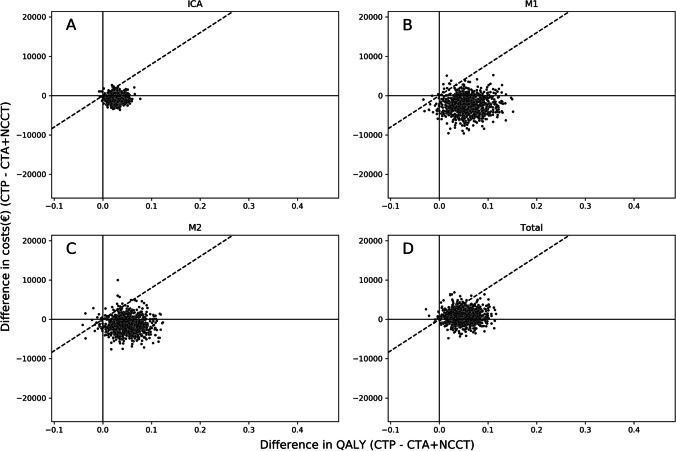
Results: We included 701 patients (median age: 72, IQR: [62-81]) years). Per LVO patient, CTP-based occlusion detection resulted in cost savings (ΔCosts median: € - 2671, IQR: [€ - 4721; € - 731]), a health gain (ΔQALY median: 0.073, IQR: [0.044; 0.104]), and a positive NMB (median: €8436, IQR: [5565; 11,876]) per LVO patient.
Conclusion: CTP-based screening of suspected stroke patients for an endovascular treatment eligible large vessel occlusion was cost-effective.
Clinical relevance statement: Although CTP-based patient selection for endovascular treatment has been recently suggested to result in worse patient outcomes after ischemic stroke, an alternative CTP-based screening for endovascular treatable occlusions is cost-effective.
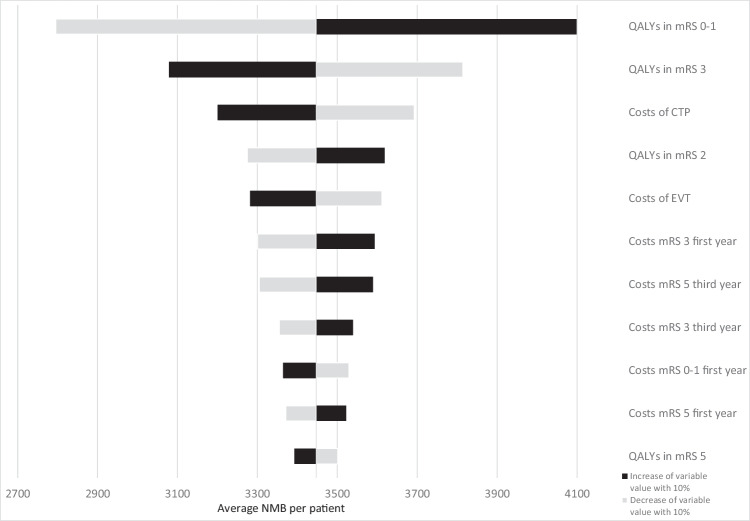
Key points: • Using CT perfusion to detect an endovascular treatment-eligible occlusions resulted in a health gain and cost savings during 10 years of follow-up. • Depending on the screening costs related to the number of patients needed to image with CT perfusion, cost savings could be considerable (median: € - 3857, IQR: [€ - 5907; € - 1916] per patient). • As the gain in quality adjusted life years was most affected by the sensitivity of CT perfusion-based occlusion detection, additional studies for the diagnostic accuracy of CT perfusion for occlusion detection are required.
Keywords: Diagnosis; Four-dimensional computed tomography; Health Care Economics and Organizations; Ischemic stroke; Thrombectomy.
© 2023. The Author(s).
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies: Codman, Stryker, AngioCare, Medtronic, Covidien, EV3, MEDAC, LAMePRO, Penumbra, Top Medical, Concentric, Nicolab, Medtronic, Cerenovus, Bracco Imaging, Servier, Genentech, Vesalio, Philips, Zoll Circulation, Insera Therapeutics.
WHvZ reports personal fees from Codman and from Stryker. DWJD report grants from the Dutch Heart Foundation, AngioCare, Medtronic/Covidien/EV3, MEDAC/LAMEPRO, Penumbra, Top Medical/Concentric, Stryker, and Cerenovus; consultation fees from Stryker, Bracco Imaging, and Servier, received by the Erasmus University Medical Centre outside this project. CBLMM reports grants from TWIN, during the conduct of the study and grants from CVON/Dutch Heart Foundation, European Commission, Dutch Health Evaluation Program, and from Stryker outside this project (paid to institution) and is shareholder of Nicolab. AJY reports Research grants from Medtronic, Cerenovus, Penumbra, Stryker, and Genentech. Consultant for Penumbra, Cerenovus, Nicolab, Philips, Vesalio, Zoll Circulation, and NIH/NINDS. YR is a shareholder of Nicolab. Equity interests in Insera Therapeutics and Nicolab. All other contributors report no conflicts of interest.
Figures

References
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49:46–110. doi: 10.1161/STR.0000000000000158. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
