

Epidemiologic profile and prevalence of live births with orofacial cleft in Brazil: a descriptive study
- PMID: 37729242
- PMCID: PMC10508041
- DOI: 10.1590/1984-0462/2024/42/2022234
Epidemiologic profile and prevalence of live births with orofacial cleft in Brazil: a descriptive study
Abstract
Objective: To describe the epidemiological profile and prevalence of live births with orofacial clefts in Brazil between 1999 and 2020.
Methods: Descriptive study. The population corresponded to live births with isolated orofacial clefts in Brazil registered in the Live Birth Information System between 1999 and 2020. Descriptive variables were selected according to their availability and grouped into socioeconomic and demographic, maternal and child health care, and biological variables. Data were submitted to a descriptive analysis using the Software for Statistics and Data Science (STATA).
Results: During the period, 33,699 children were born with orofacial clefts, and 82.1% (27,677) of them were isolated clefts. Regarding these cases, the majority were cleft lip and palate (9,619 or 34.7%), followed by cleft palate (9,442 or 34.1%), and by cleft lip (8,616 or 31.3%).
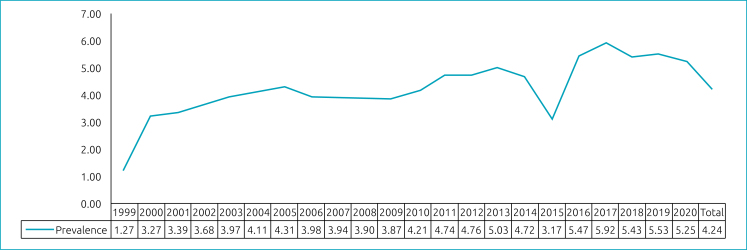
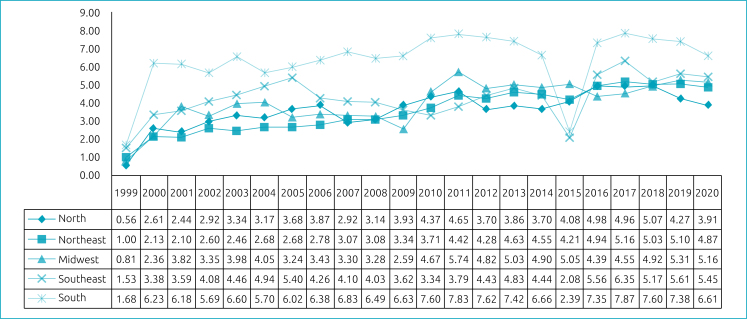
Conclusions: Live births with orofacial clefts in Brazil were male, white, with birthweight ≥2,500 g and gestational age ≥37 weeks, born by cesarean section, and with Apgar scores ≥7. The cases were more frequent among mothers who were in their first and single pregnancy and had seven or more prenatal appointments. The mothers were 20 and 29 years old, had eight to ten years of study, and were single. The national prevalence of clefts was 4.24/10,000. The South and Southeast regions of Brazil had the highest prevalence, while the lowest prevalence was recorded in the Northeast and North regions. For the Federative Units, the highest and lowest prevalences were found, respectively, in Paraná and Acre.
Objetivo:: Descrever o perfil epidemiológico e a prevalência dos nascidos vivos com fissuras orofaciais no Brasil entre 1999 e 2020.
Métodos:: Estudo descritivo. A população correspondeu aos nascidos vivos com fissuras orofaciais isoladas no Brasil registrados no Sistema de Informação de Nascidos Vivos entre 1999 e 2020. As variáveis descritivas foram selecionadas de acordo com a sua disponibilidade e agrupadas em variáveis socioeconômicas e demográficas, de atenção à saúde materno-infantil e biológicas. Os dados foram submetidos a análise descritiva utilizando o Software for Statistics and Data Science (STATA).
Resultados:: No período, 33.699 indivíduos nasceram com fissura orofacial no Brasil, e 82,1% (27.677) deles foram fissuras isoladas. Com relação a esses casos, a maioria foi de fissuras de lábio e palato (9.619 ou 34,7%), seguidas por fissura de palato (9.442 ou 34,1%) e por fissura de lábio (8.616 ou 31,1%).
Conclusões:: O perfil epidemiológico dos nascidos vivos com fissuras orofaciais no Brasil foi de nascidos do sexo masculino, da raça/cor branca, por parto cesáreo, com peso ao nascer ≥2,500 g, idade gestacional ≥37 semanas e com índices de Apgar ≥7. Os casos foram mais frequentes entre mães que estavam na primeira gestação, única e que haviam realizado sete ou mais consultas de pré-natal. As mães, com maior frequência, tinham entre 20 e 29 anos, apresentavam oito ou mais anos de estudo, eram solteiras e residiam em cidades do interior. A prevalência nacional de fissuras foi de 4,24/10.000. As Regiões Sul e Sudeste apresentaram as maiores prevalências, enquanto as menores foram registradas nas Regiões Nordeste e Norte. Para as Unidades Federativas, as maiores e menores prevalências foram encontradas, respectivamente, no Paraná e no Acre.
Conflict of interest statement
The authors declare there is no conflict of interests.
Figures
Similar articles
-
Orofacial clefts in newborns in Brazil: a time series study, 2010-2021.Epidemiol Serv Saude. 2025 May 12;34:e20240027. doi: 10.1590/S2237-96222025v34e20240027.en. eCollection 2025. Epidemiol Serv Saude. 2025. PMID: 40366940 Free PMC article.
-
Orofacial clefts in Brazil and surgical rehabilitation under the Brazilian National Health System.Braz Oral Res. 2017 Mar 30;31:e23. doi: 10.1590/1807-3107BOR-2017.vol31.0023. Braz Oral Res. 2017. PMID: 28380087
-
Demographics of orofacial clefts in Canada from 2002 to 2008.Cleft Palate Craniofac J. 2013 Mar;50(2):224-30. doi: 10.1597/10-223. Epub 2011 Sep 9. Cleft Palate Craniofac J. 2013. PMID: 21905911
-
Maternal cigarette smoking during pregnancy and the risk of having a child with cleft lip/palate.Plast Reconstr Surg. 2000 Feb;105(2):485-91. doi: 10.1097/00006534-200002000-00001. Plast Reconstr Surg. 2000. PMID: 10697150 Review.
-
Asian oral-facial cleft birth prevalence.Cleft Palate Craniofac J. 2006 Sep;43(5):580-9. doi: 10.1597/05-167. Cleft Palate Craniofac J. 2006. PMID: 16986997 Review.
Cited by
-
Orofacial clefts in newborns in Brazil: a time series study, 2010-2021.Epidemiol Serv Saude. 2025 May 12;34:e20240027. doi: 10.1590/S2237-96222025v34e20240027.en. eCollection 2025. Epidemiol Serv Saude. 2025. PMID: 40366940 Free PMC article.
-
The Global Occurrences of Cleft Lip and Palate in Pediatric Patients and Their Association with Demographic Factors: A Narrative Review.Children (Basel). 2024 Mar 8;11(3):322. doi: 10.3390/children11030322. Children (Basel). 2024. PMID: 38539356 Free PMC article. Review.
References
-
- Nagappan N, John J. Sociodemographic profile of orofacial cleft patients in India: a hospital-based study. Int J Med Public Health. 2015;5:35–39. doi: 10.4103/2230-8598.151253. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
