

Axillary to Radial Nerve Transfer for Recovery of Elbow Extension After Spinal Cord Injury
- PMID: 37729631
- PMCID: PMC12245348
- DOI: 10.1227/ons.0000000000000885
Axillary to Radial Nerve Transfer for Recovery of Elbow Extension After Spinal Cord Injury
Abstract
Background and objectives: Cervical spinal cord injuries (SCI) result in severe loss of function and independence. Nerve transfers have become a powerful method for restoring upper extremity function, the most critical missing function desired by this patient population. Recovery of active elbow extension allows for expansion of one's workspace to reach for objects and stabilizes control at the elbow joint. Without triceps function, a patient with a cervical SCI is rendered entirely helpless when in the supine position. Our objective was to provide a concise description of the transfer of branches of the axillary nerve (AN) to the long head of the triceps branch of the radial nerve (RN) for restoration of elbow extension after cervical SCI.
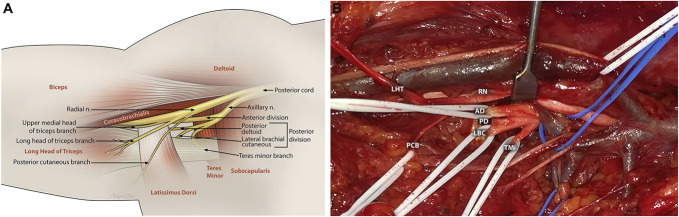
Methods: An anterior, axillary approach is used for the transfer of the nerve branches of the AN (which may include branches to the teres minor, posterior deltoid, or even middle deltoid) to the long head of the triceps branch of the RN. Preoperative assessment and intraoperative stimulation are demonstrated to direct optimal selection of axillary branch donors.
Results: The axillary approach provides full access to all branches of the AN in optimal proximity to triceps branches of the RN and allows for tension-free coaptation to achieve successful recovery of elbow extension. Final outcomes may not be achieved for 18 months. Of our last 20 patients with greater than 12-month follow-up, 13 have achieved antigravity strength in elbow extension, 4 are demonstrating ongoing progression, and 3 are definitive failures by 18 months.
Conclusion: The axillary to RN transfer is an important intervention for recovery of elbow extension after cervical SCI, which significantly improves quality of life in this patient population. Further large population outcomes studies are necessary to further establish efficacy and increase awareness of these procedures.
Copyright © Congress of Neurological Surgeons 2023. All rights reserved.
Figures

Similar articles
-
Modified Partial Radial to Axillary Nerve Transfer.JBJS Essent Surg Tech. 2025 Jun 25;15(2):e22.00026. doi: 10.2106/JBJS.ST.22.00026. eCollection 2025 Apr-Jun. JBJS Essent Surg Tech. 2025. PMID: 40567509 Free PMC article.
-
Transfer of the Intercostal Nerves to the Radial Nerve Branch Innervating the Long Head of the Triceps Muscle for Elbow Extension.JBJS Essent Surg Tech. 2025 Aug 25;15(3):e23.00092. doi: 10.2106/JBJS.ST.23.00092. eCollection 2025 Jul-Sep. JBJS Essent Surg Tech. 2025. PMID: 40861031 Free PMC article.
-
Gracilis Free Flap Technique for Elbow Flexion Reconstruction.JBJS Essent Surg Tech. 2025 Jul 17;15(3):e25.00003. doi: 10.2106/JBJS.ST.25.00003. eCollection 2025 Jul-Sep. JBJS Essent Surg Tech. 2025. PMID: 40678176 Free PMC article.
-
Upper extremity nerve transfers for acute flaccid myelitis: a systematic literature review.Childs Nerv Syst. 2022 Mar;38(3):521-526. doi: 10.1007/s00381-021-05419-x. Epub 2022 Jan 4. Childs Nerv Syst. 2022. PMID: 34982205
-
Manipulative interventions for reducing pulled elbow in young children.Cochrane Database Syst Rev. 2017 Jul 28;7(7):CD007759. doi: 10.1002/14651858.CD007759.pub4. Cochrane Database Syst Rev. 2017. PMID: 28753234 Free PMC article.
References
-
- Anderson KD. Targeting recovery: priorities of the spinal cord-injured population. J Neurotrauma. 2004;21(10):1371-1383. - PubMed
-
- Bazarek S, Brown JM. The evolution of nerve transfers for spinal cord injury. Exp Neurol. 2020;333:113426. - PubMed
-
- Bertelli JA, Kechele PR, Santos MA, Duarte H, Ghizoni MF. Axillary nerve repair by triceps motor branch transfer through an axillary access: anatomical basis and clinical results. J Neurosurg. 2007;107(2):370-377. - PubMed
-
- Bertelli JA, Santos MA, Kechele PR, Ghizoni MF, Duarte H. Triceps motor nerve branches as a donor or receiver in nerve transfers. Neurosurgery. 2007;61(5):333-339; discussion 338-339. - PubMed
-
- Bertelli JA, Goklani MS, Patel N, Duarte ECW. Triceps and cutaneous radial nerve branches investigated via an axillary anterior arm approach: new findings in a fresh-cadaver anatomical study. J Neurosurg. 2022;136(5):1424-1433. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
