

Spatially aware deep learning reveals tumor heterogeneity patterns that encode distinct kidney cancer states
- PMID: 37729872
- PMCID: PMC10518628
- DOI: 10.1016/j.xcrm.2023.101189
Spatially aware deep learning reveals tumor heterogeneity patterns that encode distinct kidney cancer states
Abstract
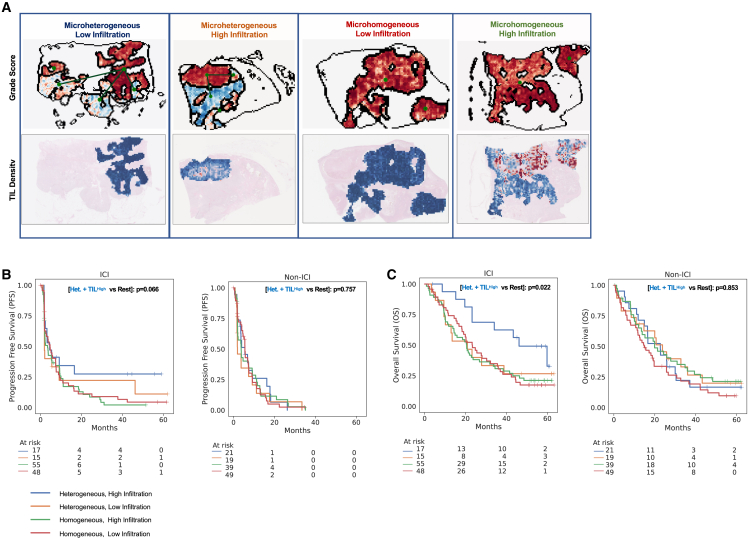
Clear cell renal cell carcinoma (ccRCC) is molecularly heterogeneous, immune infiltrated, and selectively sensitive to immune checkpoint inhibition (ICI). However, the joint tumor-immune states that mediate ICI response remain elusive. We develop spatially aware deep-learning models of tumor and immune features to learn representations of ccRCC tumors using diagnostic whole-slide images (WSIs) in untreated and treated contexts (n = 1,102 patients). We identify patterns of grade heterogeneity in WSIs not achievable through human pathologist analysis, and these graph-based "microheterogeneity" structures associate with PBRM1 loss of function and with patient outcomes. Joint analysis of tumor phenotypes and immune infiltration identifies a subpopulation of highly infiltrated, microheterogeneous tumors responsive to ICI. In paired multiplex immunofluorescence images of ccRCC, microheterogeneity associates with greater PD1 activation in CD8+ lymphocytes and increased tumor-immune interactions. Our work reveals spatially interacting tumor-immune structures underlying ccRCC biology that may also inform selective response to ICI.
Keywords: AI; artificial intelligence; computational histopathology; computer vision; deep learning; immunotherapy; kidney cancer; precision medicine; tumor heterogeneity.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests T.K.C. reports institutional and personal paid and unpaid support for research, advisory boards, consultancy, and honoraria from Alkermes, AstraZeneca, Aravive, Aveo, Bayer, Bristol Myers-Squibb, Calithera, Circle Pharma, Deciphera Pharmaceuticals, Eisai, EMD Serono, Exelixis, GlaxoSmithKline, Gilead, IQVA, Infinity, Ipsen, Jansen, Kanaph, Lilly, Merck, Nikang, Nuscan, Novartis, Oncohost, Pfizer, Roche, Sanofi/Aventis, Scholar Rock, Surface Oncology, Takeda, Tempest, UpToDate, and CME events (Peerview, OncLive, MJH, CCO, and others), outside the submitted work; institutional patents filed on molecular alterations and immunotherapy response/toxicity and ctDNA; and equity in Tempest, Pionyr, Osel, Precede Bio, CureResponse, and InnDura. T.K.C. serves on the committees of NCCN, GU Steering Committee, and ASCO/ESMO. Medical writing and editorial assistance support may have been funded by communications companies in part. T.K.C. does not report any speaker’s bureau. T.K.C. has mentored several non-US citizens on research projects with potential funding (in part) from non-US sources/foreign components. The institution (Dana-Farber Cancer Institute) may have received additional independent funding of drug companies and/or royalties potentially involved in research around the subject matter. E.M.V.A. reports advisory/consulting with Tango Therapeutics, Genome Medical, Invitae, Monte Rosa, Enara Bio, Manifold Bio, Riva Therapeutics, Serinus Bio, and Janssen; research support from Novartis and BMS; equity in Tango Therapeutics, Genome Medical, Syapse, Manifold Bio, Monte Rosa, Enara Bio, Riva Therapeutics, and Serinus Bio; institutional patents filed on chromatin mutations and immunotherapy response and on methods for clinical interpretation; and intermittent legal consulting on patents for Foaley & Hoag. D.A.B. reports personal fees from LM Education and Exchange, Adnovate Strategies, MDedge, Cancer Network, Cancer Expert Now, OncLive, Catenion, and AVEO and grants and personal fees from Exelixis outside the submitted work. C.L. reports research funding from Genentech/imCORE. Z.B. reports research funding from Bristol-Myers Squibb and Genentech/imCORE and honoraria from UpToDate. S.S. reports grants from Exelixis, grants from Bristol-Myers Squibb, personal fees from Merck, grants and personal fees from AstraZeneca, personal fees from CRISPR Therapeutics, personal fees from NCI, and personal fees from AACR as well as a patent for Biogenex with royalties paid. K.B. has consulted for Related Sciences (RS) outside of the scope of this work. S.R. receives research funding from Bristol-Myers Squibb and KITE/Gilead and is a member of the SAB for Immunitas Therapeutics.
Figures






Update of
-
Spatially aware deep learning reveals tumor heterogeneity patterns that encode distinct kidney cancer states.bioRxiv [Preprint]. 2023 Feb 20:2023.01.18.524545. doi: 10.1101/2023.01.18.524545. bioRxiv. 2023. Update in: Cell Rep Med. 2023 Sep 19;4(9):101189. doi: 10.1016/j.xcrm.2023.101189. PMID: 36712053 Free PMC article. Updated. Preprint.
References
-
- Gerlinger M., Rowan A.J., Horswell S., Math M., Larkin J., Endesfelder D., Gronroos E., Martinez P., Matthews N., Stewart A., et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N. Engl. J. Med. 2012;366:883–892. doi: 10.1056/NEJMoa1113205. - DOI - PMC - PubMed
-
- Mitchell T.J., Turajlic S., Rowan A., Nicol D., Farmery J.H.R., O'Brien T., Martincorena I., Tarpey P., Angelopoulos N., Yates L.R., et al. Timing the Landmark Events in the Evolution of Clear Cell Renal Cell Cancer: TRACERx Renal. Cell. 2018;173:611–623.e17. doi: 10.1016/j.cell.2018.02.020. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
