

Perampanel's forgiveness factor in a variable medication adherence paradigm in a rat model of chronic epilepsy
- PMID: 37730661
- PMCID: PMC10510183
- DOI: 10.1186/s12967-023-04490-z
Perampanel's forgiveness factor in a variable medication adherence paradigm in a rat model of chronic epilepsy
Abstract
Background: Poor medication adherence contributes to increased morbidity and mortality in patients with epilepsy and may be under-addressed in clinical practice. Ethical concerns make it impossible to study the impact of medication nonadherence in clinical trials, but our previous work emphasizes the importance of using preclinical approaches to address these questions. With over 30 clinically available antiseizure medicines (ASM's), it remains an important question to understand the relationship between poor adherence and seizure incidence across mechanistically distinct ASM's, including the broad-spectrum ASM, perampanel (PER).
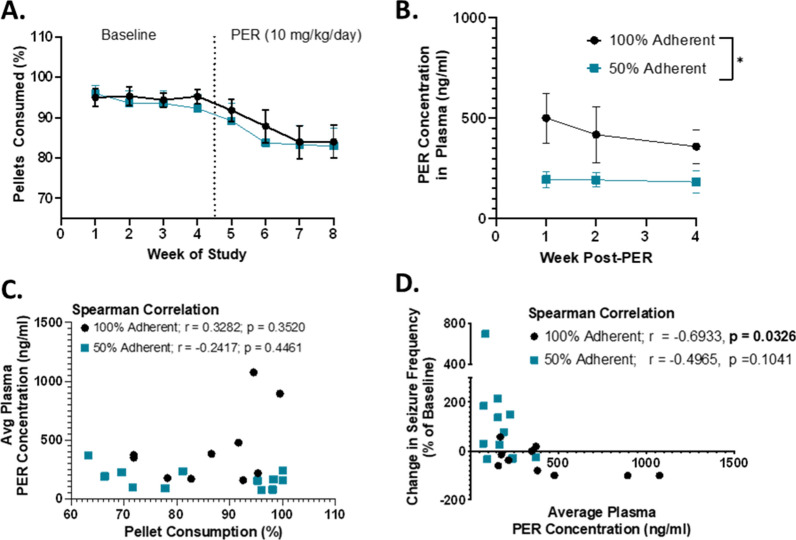
Methods: We formulated PER into chow pellets to deliver to rats in a 100% fully adherent or 50% variable nonadherent paradigm via our novel automated medication-in-food delivery system. Chronic oral dosing was initiated in male rats with chronic epilepsy while monitoring 24/7 for videoEEG evidence of seizures during a 4-week placebo baseline and 4-week treatment phase. PER concentrations were monitored in plasma at 1-week intervals and correlated with degree of seizure control. The relationship between missed doses and extended patterns of nonadherence were correlated with breakthrough seizures.
Results: Fully adherent rats demonstrated a median reduction in seizure frequency of 50%, whereas nonadherent rats had a median increase of 54%. Plasma concentrations of PER were stable over the 4-week treatment period in both fully adherent and nonadherent groups, with levels being twice as high in fully adherent animals. There was no correlation between a single missed dose or series of missed doses and the incidence of breakthrough seizures. However, those animals in the nonadherent group that received PER for every meal during a 24-h period had a reduced likelihood of seizure incidence.
Conclusions: If our preclinical data is supported in the clinic, PER's favorable pharmacokinetic profile in humans, combined with a lowered risk of breakthrough seizures suggests that it may provide a certain forgiveness factor if a dose is missed within a 24-h window.
Keywords: Adherence; Antiseizure medicine; Breakthrough seizures; Epilepsy; Perampanel.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures




Similar articles
-
Temporal relationship between levetiracetam nonadherence and breakthrough seizures in a preclinical model of temporal lobe epilepsy.Epilepsia. 2024 Feb;65(2):497-510. doi: 10.1111/epi.17835. Epub 2023 Dec 12. Epilepsia. 2024. PMID: 38031477
-
Correction of medication nonadherence results in better seizure outcomes than dose escalation in a novel preclinical epilepsy model of adherence.Epilepsia. 2019 Mar;60(3):475-484. doi: 10.1111/epi.14655. Epub 2019 Jan 22. Epilepsia. 2019. PMID: 30669183
-
Adherence to antiseizure medications in an underserved population with epilepsy.Epilepsy Behav. 2023 Dec;149:109484. doi: 10.1016/j.yebeh.2023.109484. Epub 2023 Nov 20. Epilepsy Behav. 2023. PMID: 37988904
-
Perampanel: Does it have broad-spectrum potential?Epilepsia. 2019 Mar;60 Suppl 1:22-36. doi: 10.1111/epi.14456. Epub 2018 Jun 28. Epilepsia. 2019. PMID: 29953584 Review.
-
Extended-release formulations for the treatment of epilepsy.CNS Drugs. 2007;21(9):765-74. doi: 10.2165/00023210-200721090-00005. CNS Drugs. 2007. PMID: 17696575 Review.
Cited by
-
BDNF/Cyclin D1 Signaling System and Cognitive Performance After Perampanel and Lacosamide Treatment Singly or in Combination in an Experimental Model of Temporal Lobe Epilepsy.Curr Issues Mol Biol. 2024 Dec 11;46(12):14010-14032. doi: 10.3390/cimb46120838. Curr Issues Mol Biol. 2024. PMID: 39727966 Free PMC article.
-
Technological Vanguard: the outstanding performance of the LTY-CNN model for the early prediction of epileptic seizures.J Transl Med. 2024 Feb 16;22(1):162. doi: 10.1186/s12967-024-04945-x. J Transl Med. 2024. PMID: 38365732 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
