

Large T cell clones expressing immune checkpoints increase during multiple myeloma evolution and predict treatment resistance
- PMID: 37730678
- PMCID: PMC10511411
- DOI: 10.1038/s41467-023-41562-6
Large T cell clones expressing immune checkpoints increase during multiple myeloma evolution and predict treatment resistance
Abstract
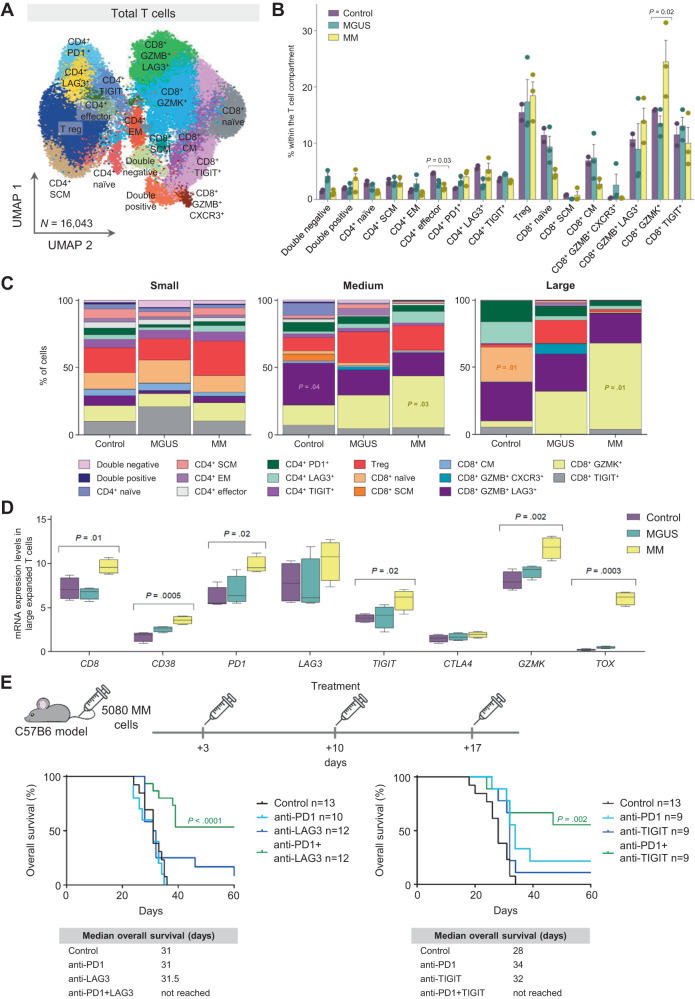
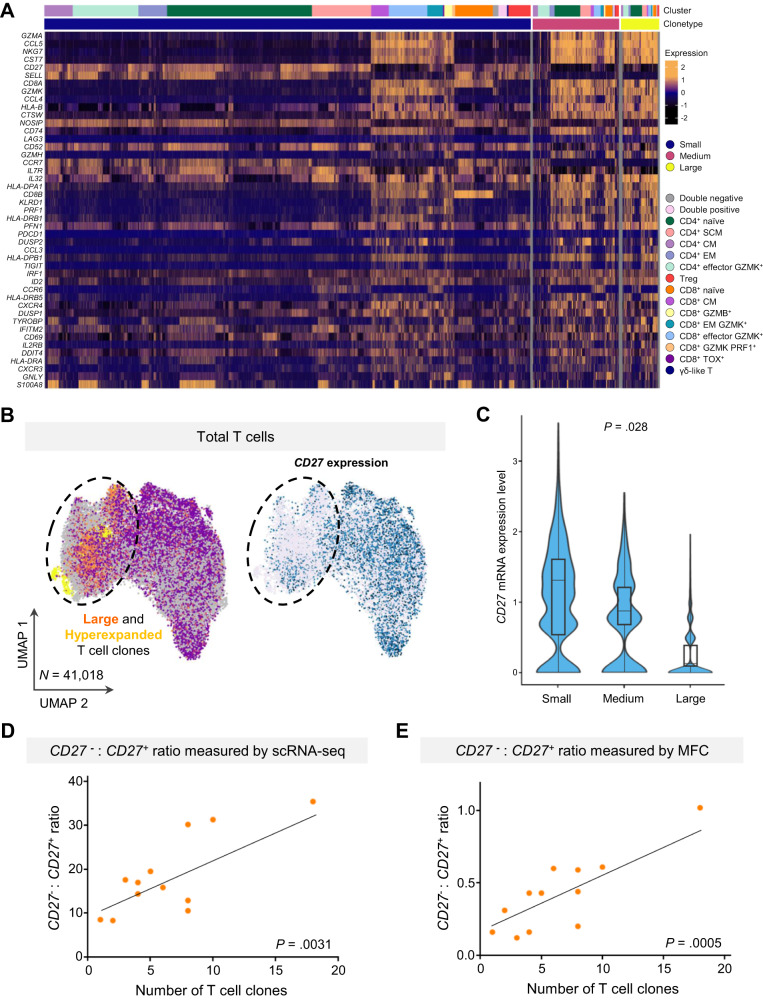
Tumor recognition by T cells is essential for antitumor immunity. A comprehensive characterization of T cell diversity may be key to understanding the success of immunomodulatory drugs and failure of PD-1 blockade in tumors such as multiple myeloma (MM). Here, we use single-cell RNA and T cell receptor sequencing to characterize bone marrow T cells from healthy adults (n = 4) and patients with precursor (n = 8) and full-blown MM (n = 10). Large T cell clones from patients with MM expressed multiple immune checkpoints, suggesting a potentially dysfunctional phenotype. Dual targeting of PD-1 + LAG3 or PD-1 + TIGIT partially restored their function in mice with MM. We identify phenotypic hallmarks of large intratumoral T cell clones, and demonstrate that the CD27- and CD27+ T cell ratio, measured by flow cytometry, may serve as a surrogate of clonal T cell expansions and an independent prognostic factor in 543 patients with MM treated with lenalidomide-based treatment combinations.
© 2023. Springer Nature Limited.
Conflict of interest statement
C.B. has served as a member on advisory boards for Amgen, Janssen, Pfizer, Takeda, and Oncopeptides; A.R. has received honoraria from Amgen, Celgene, and Janssen and a research grant from AstraZeneca and the Associazione Italiana per la Ricerca sul Cancro (AIRC): AIRC-IG-24689. H.G. has received speakers bureau honoraria from Academy2, KG, Agentur Hogg Robinson Germany, Amgen, ArtTempi, Beupdated Helbig Consulting and Research AG Schweiz, Bristol Myers Squibb, Celgene, Chop, Chugai, Congress Culture Concept Dr. S. Stocker München, Connectmedia Warschau/Polen, Dr. Hubmann Tumorzentrum München, FomF, GlaxoSmithKline, GWT Forschung und Innovation Dresden, Institut für Versorgungsforschung in der Onkologie GbR, Janssen, Kompetenznetz Maligne Lymphome, MedConcept, Medical Communication, Münchner Leukämie Labor Prof. Haferlach, New Concept Oncology, Novartis, Omnia Med Deutschland, Onko Internetportal DKG-web, Sanofi, STIL Forschungs, and Veranstaltungskonzept Gesundheit Mechernich, has served as a member on advisory boards for Adaptive Biotechnology, Amgen, Bristol Myers Squibb, Celgene, Janssen, Sanofi, and Takeda, and has received research grants and/or materials such as investigational medicinal products from Amgen, Bristol Myers Squibb, Celgene, Chugai, Dietmar-Hopp-Foundation, Janssen, John Hopkins University, and Sanofi. A. Oriol participated in advisory boards for Amgen, Celgene and Janssen. M.-V.M. has received honoraria for lectures from or participated in advisory boards for Janssen, Celgene, Amgen, Takeda, AbbVie, Adaptive, GSK, Pharmamar, EDO, and Oncopeptides. L.R. reports honoraria from Janssen, Celgene, Amgen, and Takeda. J.B. reports honoraria for lectures from Janssen, Amgen, Celgene, Takeda, and Oncopeptides. J.-J.L. reports honoraria from and membership on boards of directors or advisory committees with Takeda, Amgen, Celgene, and Janssen. J.F.S.-M. reports consultancy for Bristol-Myers Squibb, Celgene, Novartis, Takeda, Amgen, MSD, Janssen, and Sanofi and membership on a board of directors or advisory committee with Takeda. J.A.M.-C. has received research grants from Roche, Bristol-Myers Squibb-Celgene, and Janssen. B.P. reports honoraria for lectures from and membership on advisory boards with Adaptive, Amgen, Becton Dickinson, Bristol-Myers Squibb-Celgene, Janssen, Merck, Novartis, Roche, Sanofi and Takeda; unrestricted grants from Bristol-Myers Squibb-Celgene, EngMab, Roche, Sanofi, and Takeda; and consultancy for Bristol-Myers Squibb-Celgene, Janssen, Sanofi, and Takeda. The remaining authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
