

Evidence of a causal and modifiable relationship between kidney function and circulating trimethylamine N-oxide
- PMID: 37730687
- PMCID: PMC10511707
- DOI: 10.1038/s41467-023-39824-4
Evidence of a causal and modifiable relationship between kidney function and circulating trimethylamine N-oxide
Abstract
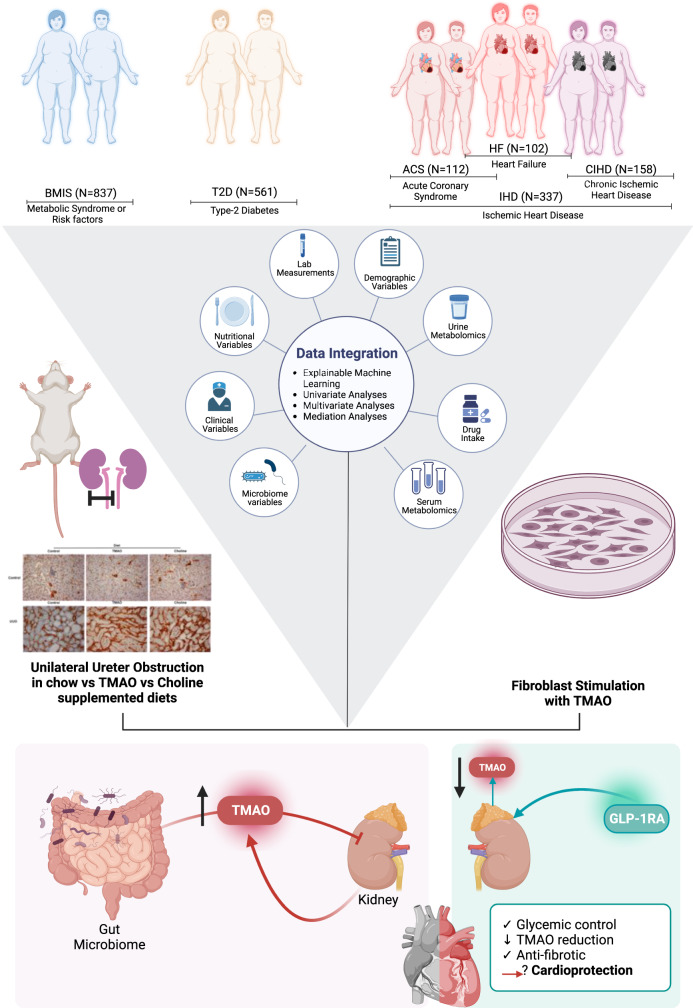
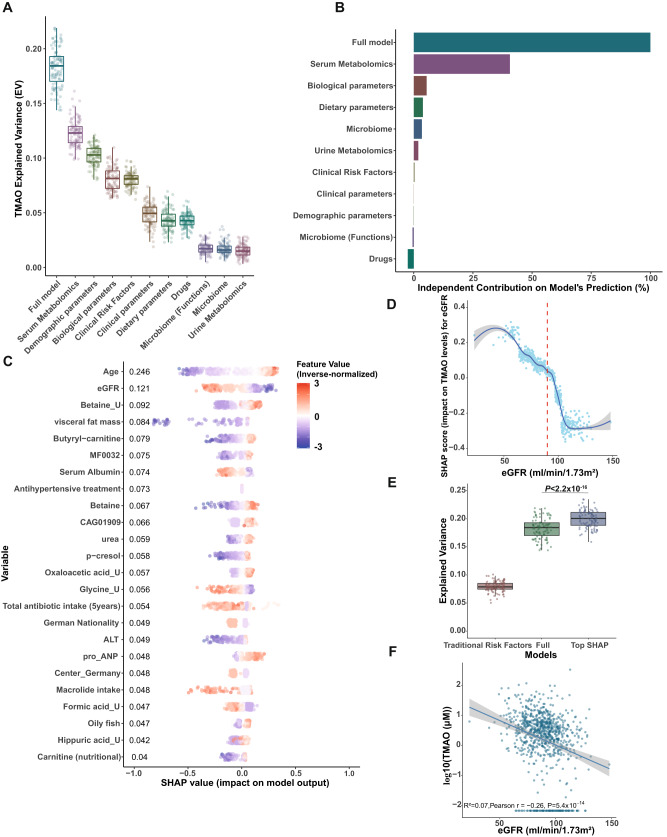
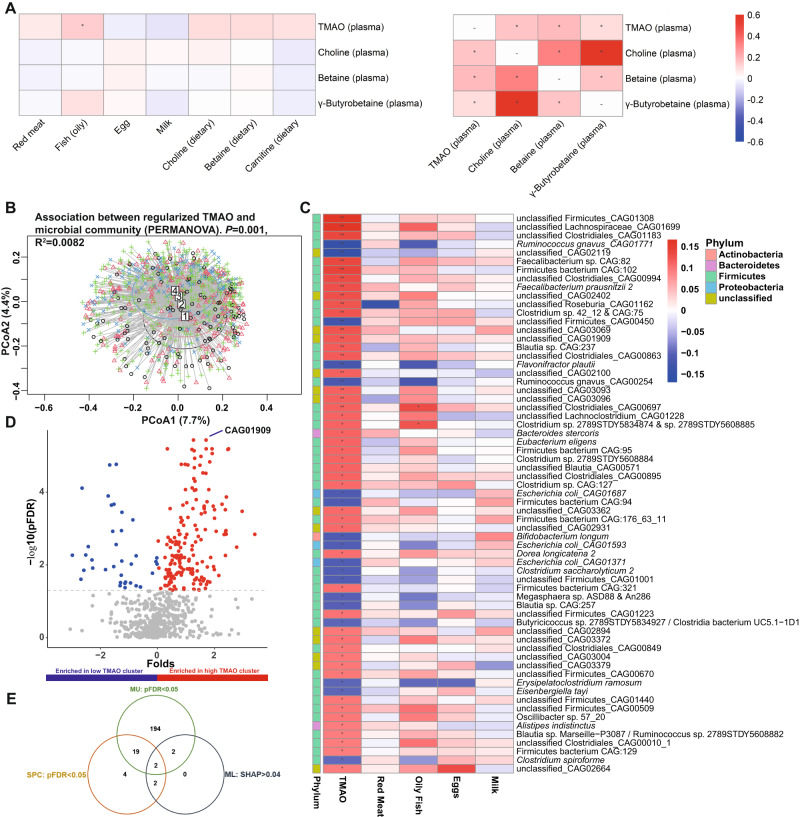
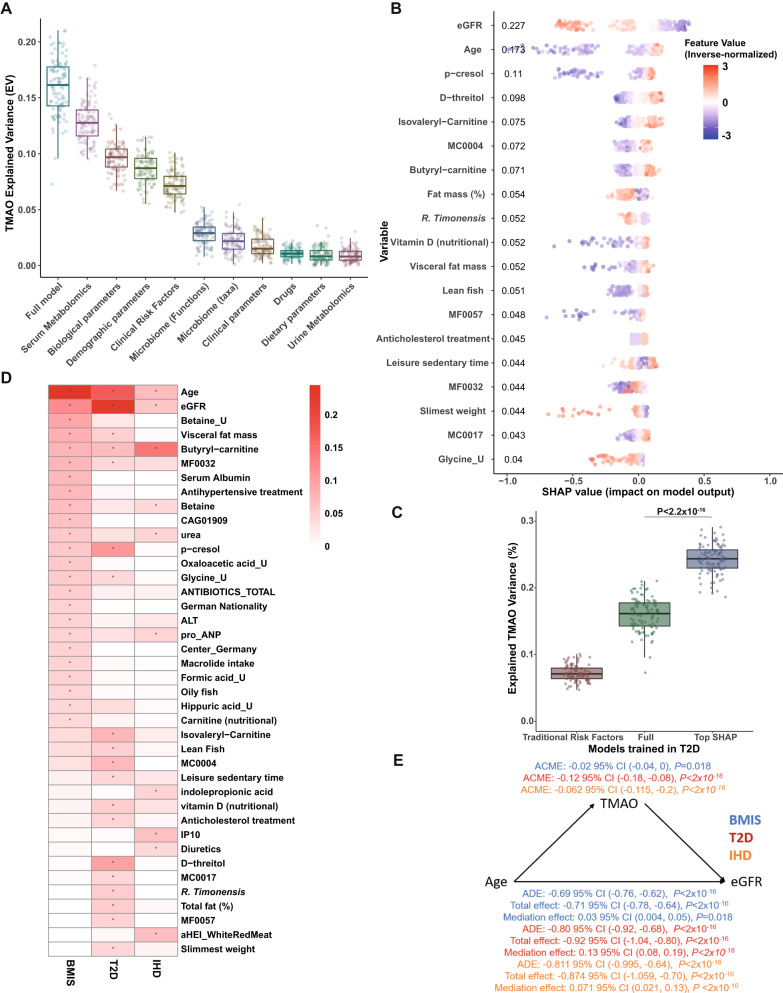
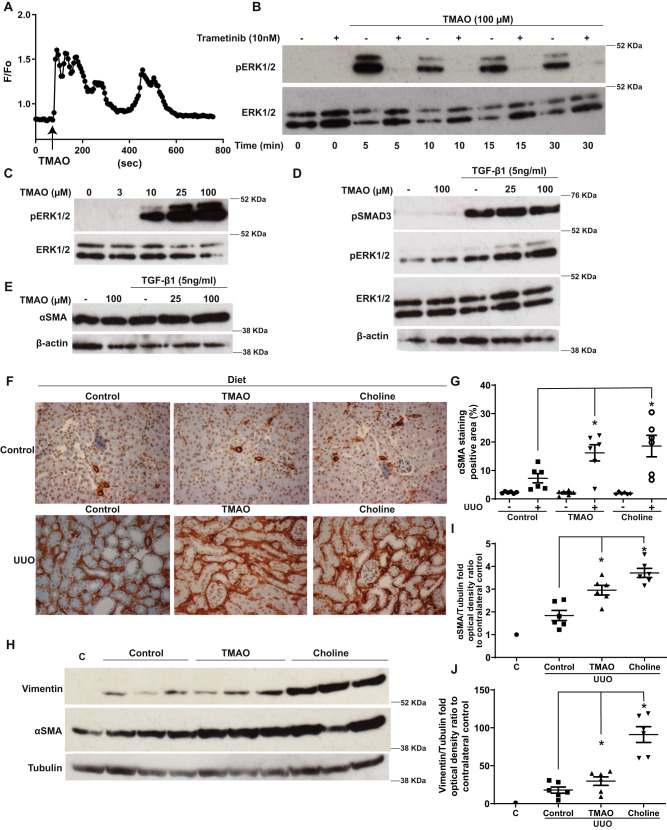
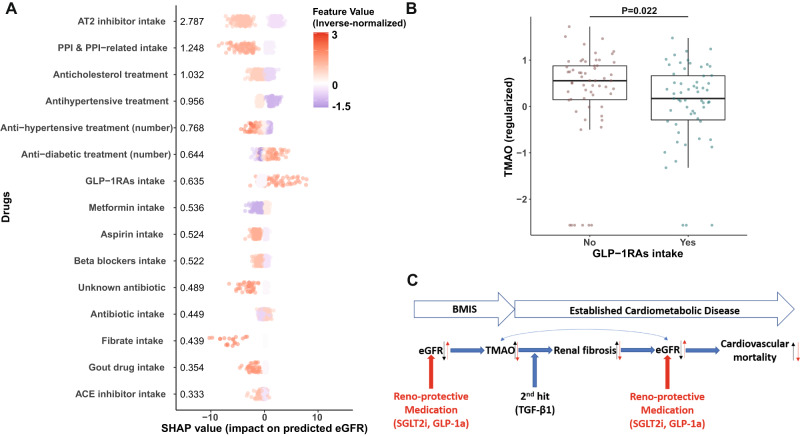
The host-microbiota co-metabolite trimethylamine N-oxide (TMAO) is linked to increased cardiovascular risk but how its circulating levels are regulated remains unclear. We applied "explainable" machine learning, univariate, multivariate and mediation analyses of fasting plasma TMAO concentration and a multitude of phenotypes in 1,741 adult Europeans of the MetaCardis study. Here we show that next to age, kidney function is the primary variable predicting circulating TMAO, with microbiota composition and diet playing minor, albeit significant, roles. Mediation analysis suggests a causal relationship between TMAO and kidney function that we corroborate in preclinical models where TMAO exposure increases kidney scarring. Consistent with our findings, patients receiving glucose-lowering drugs with reno-protective properties have significantly lower circulating TMAO when compared to propensity-score matched control individuals. Our analyses uncover a bidirectional relationship between kidney function and TMAO that can potentially be modified by reno-protective anti-diabetic drugs and suggest a clinically actionable intervention for decreasing TMAO-associated excess cardiovascular risk.
© 2023. Springer Nature Limited.
Conflict of interest statement
K.C. is a consultant for Danone Research, Ysopia, and CONFO therapeutics for work not associated with this study. K.C. held a collaborative research contract with Danone Research in the context of MetaCardis project. F.B. is a shareholder of Implexion Pharma AB. M.B. received lecture and/or consultancy fees from AstraZeneca, Boehringer-Ingelheim, Lilly, Novo Nordisk, Novartis, and Sanofi. The remaining authors declare no competing interests.
Figures
References
-
- Fan Y, Pedersen O. Gut microbiota in human metabolic health and disease. Nat. Rev. Microbiol. 2021;19:55–71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
