

Understanding and treatment of cutaneous graft-versus-host-disease
- PMID: 37730800
- PMCID: PMC11759061
- DOI: 10.1038/s41409-023-02109-x
Understanding and treatment of cutaneous graft-versus-host-disease
Abstract
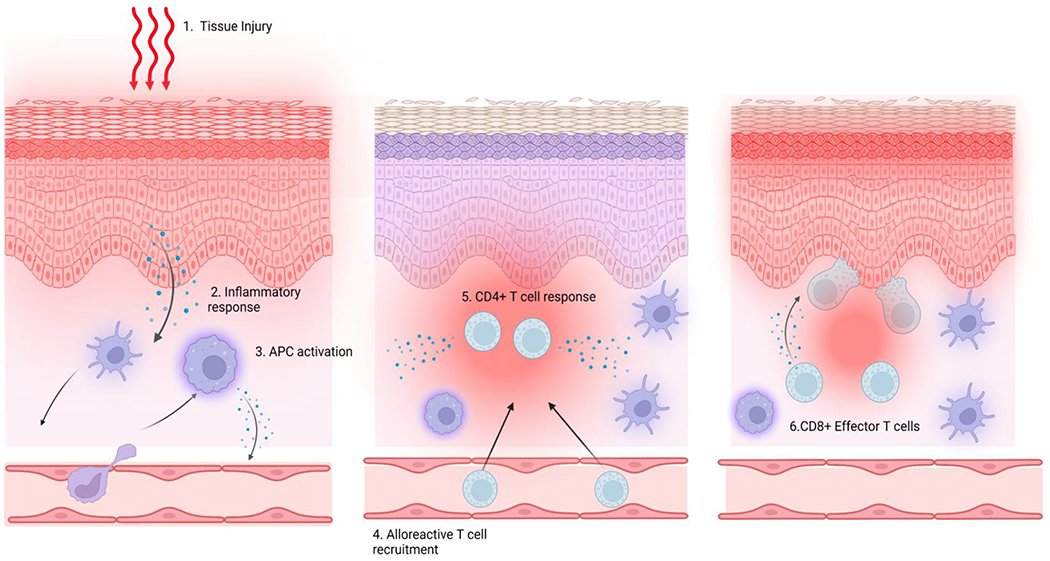
The skin is the outermost mechanical barrier where dynamic immune reactions take place and is the most commonly affected site in both acute and chronic graft-versus-host disease (GVHD). If not properly treated, pain and pruritis resulting from cutaneous GVHD can increase the risk of secondary infection due to erosions, ulcerations, and damage of underlying tissues. Furthermore, resulting disfiguration can cause distress and significantly impact patients' quality of life. Thus, a deeper understanding of skin-specific findings of GVHD is needed. This review will highlight some promising results of recent pre-clinical studies on the pathophysiology of skin GVHD and summarize the diagnostic and staging/grading procedures according to the clinical manifestations of skin GVHD. In addition, we will summarize outcomes of various GVHD treatments, including skin-specific response rates.
© 2023. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
TKK has received a research funding from Nextcure, that is not relevant to this manuscript. TKK is a consultant for Agenus and Immunobiome. ERT has previously received as a consultant for Incyte. CLK has serviced on an advisory board for Horizon Therapeutics.
Other authors declare no competing financial interests.
Figures







References
-
- Penack O, Marchetti M, Ruutu T, Aljurf M, Bacigalupo A, Bonifazi F, et al. Prophylaxis and management of graft versus host disease after stem-cell transplantation for haematological malignancies: updated consensus recommendations of the European Society for Blood and Marrow Transplantation. Lancet Haematol. 2020;7:e157–e67. - PubMed
-
- Shlomchik WD. Graft-versus-host disease. Nat Rev Immunol. 2007;7:340–52. - PubMed
-
- Hillen U, Hausermann P, Massi D, Janin A, Wolff D, Lawitschka A, et al. Consensus on performing skin biopsies, laboratory workup, evaluation of tissue samples and reporting of the results in patients with suspected cutaneous graft-versus-host disease. J Eur Acad Dermatol Venereol. 2015;29:948–54. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
