

Conservative versus early surgical treatment in the management of pyogenic spondylodiscitis: a systematic review and meta-analysis
- PMID: 37730826
- PMCID: PMC10511402
- DOI: 10.1038/s41598-023-41381-1
Conservative versus early surgical treatment in the management of pyogenic spondylodiscitis: a systematic review and meta-analysis
Abstract
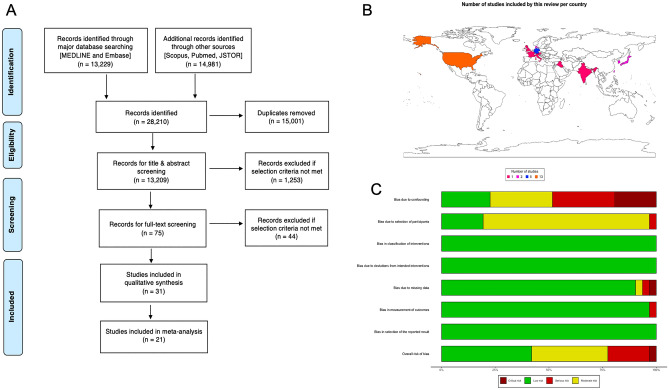
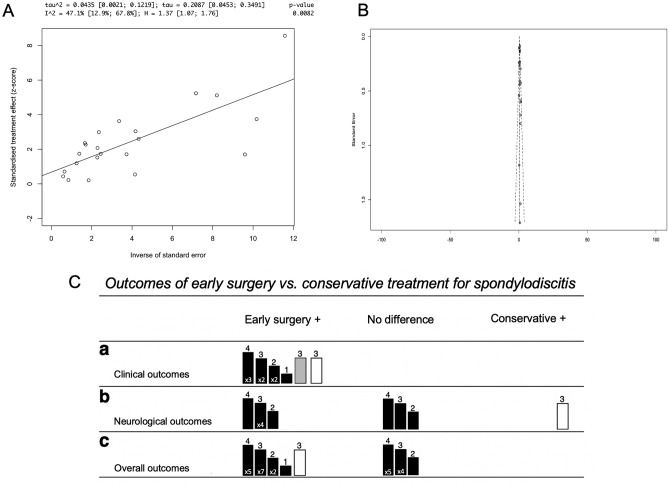
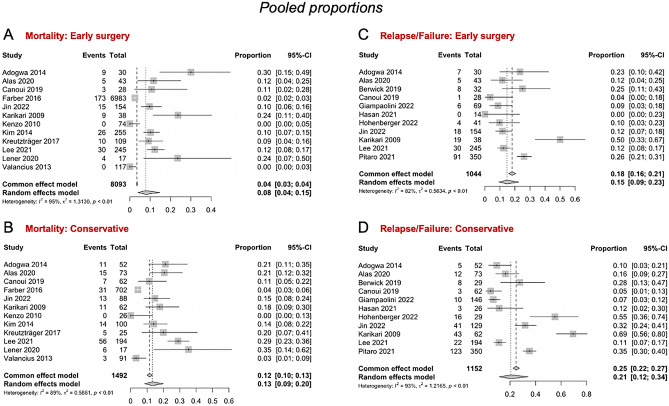
Spondylodiscitis is the commonest spine infection, and pyogenic spondylodiscitis is the most common subtype. Whilst antibiotic therapy is the mainstay of treatment, some advocate that early surgery can improve mortality, relapse rates, and length of stay. Given that the condition carries a high mortality rate of up to 20%, the most effective treatment must be identified. We aimed to compare the mortality, relapse rate, and length of hospital stay of conservative versus early surgical treatment of pyogenic spondylodiscitis. All major databases were searched for original studies, which were evaluated using a qualitative synthesis, meta-analyses, influence, and regression analyses. The meta-analysis, with an overall pooled sample size of 10,954 patients from 21 studies, found that the pooled mortality among the early surgery patient subgroup was 8% versus 13% for patients treated conservatively. The mean proportion of relapse/failure among the early surgery subgroup was 15% versus 21% for the conservative treatment subgroup. Further, it concluded that early surgical treatment, when compared to conservative management, is associated with a 40% and 39% risk reduction in relapse/failure rate and mortality rate, respectively, and a 7.75 days per patient reduction in length of hospital stay (p < 0.01). The meta-analysis demonstrated that early surgical intervention consistently significantly outperforms conservative management in relapse/failure and mortality rates, and length of stay, in patients with pyogenic spondylodiscitis.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Thavarajasingam SG, Subbiah Ponniah H, Philipps R, Neuhoff J, Kramer A, Demetriades AK, Shiban E, Ringel F, Davies BM. Increasing incidence of spondylodiscitis in England: An analysis of the national health service (NHS) hospital episode statistics from 2012 to 2021. Brain Spine J. 2023;3:1. - PMC - PubMed
-
- Gouliouris T, Aliyu SH, Brown NM. Spondylodiscitis: Update on diagnosis and management. J. Antimicrob. Chemother. 2010;65(3):11–24. - PubMed
-
- Zimmerli W. Vertebral osteomyelitis. N. Engl. J. Med. 2010;362(11):1022–1029. - PubMed
-
- Castilla JM, Martin V, Rodriguez-Salazar A. Surgical treatment of patients with spinal infection. Neurocirugia (Asturias, Spain). 2002;13(2):101–109. - PubMed
-
- Kehrer M, Pedersen C, Jensen TG, Hallas J, Lassen AT. Increased short-and long-term mortality among patients with infectious spondylodiscitis compared with a reference population. Spine J. 2015;15(6):1233–1240. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
