

Neurosurgical treatment of pediatric brain tumors - results from a single center multidisciplinary setup
- PMID: 37730915
- PMCID: PMC10837233
- DOI: 10.1007/s00381-023-06123-8
Neurosurgical treatment of pediatric brain tumors - results from a single center multidisciplinary setup
Abstract
Objective: The challenge of pediatric brain tumor surgery is given due to a relative low prevalence but high heterogeneity in age, localization, and pathology. Improvements of long-term overall survival rates were achieved during the past decades stressing the importance of a multidisciplinary decision process guided by a national treatment protocol. We reviewed the entire spectrum of pediatric brain tumor surgeries from the perspective of an interdisciplinary pediatric neuro-oncology center in Germany.
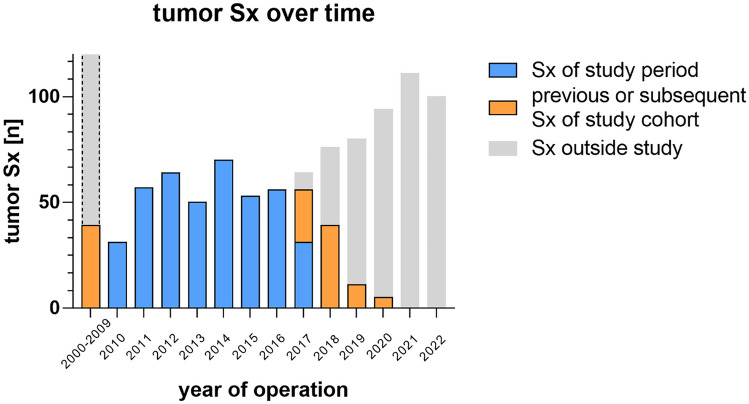
Methods: Every patient who underwent brain tumor surgery from January 2010 to June 2017 in our Pediatric Neurosurgery department was retrospectively included and evaluated regarding the course of treatment. Perioperative data such as tumor localization, timing of surgery, extent of resection, neuropathological diagnosis, transfusion rates, oncologic and radiation therapy, and neurological follow-up including morbidity and mortality were evaluated.
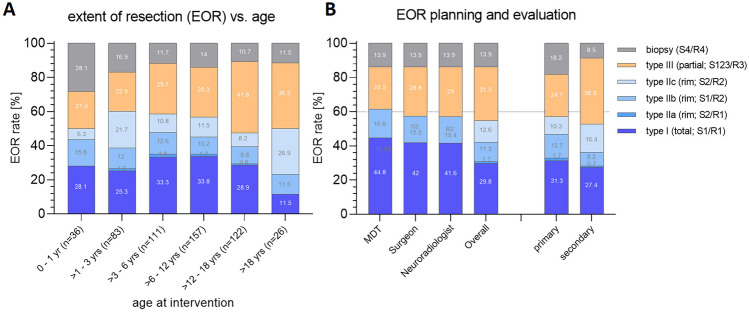
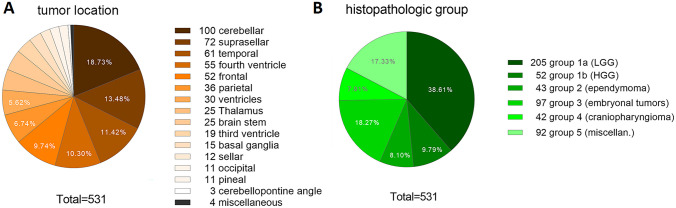
Results: Two hundred ninety-three pediatric brain tumor patients were applicable (age: 8.28 ± 5.62 years, 1.22:1.0 m:f). A total of 531 tumor surgical interventions was performed within these patients (457 tumor resections, 74 tumor biopsies; mean interventions per patient 1.8 ± 1.2). Due to a critical neurologic status, 32 operations (6%) were performed on the day of admission. In 65.2% of all cases, tumor were approached supratentorially. Most frequent diagnoses of the cases were glial tumors (47.8%) and embryonal tumors (17.6%). Preoperative planned extent of resection was achieved in 92.7%. Pre- and postoperative neurologic deficits resolved completely in 30.7%, whereas symptom regressed in 28.6% of surgical interventions. New postoperative neurologic deficit was observed in 10.7%, which resolved or improved in 80% of these cases during 30 days. The mortality rate was 1%.
Conclusion: We outlined the center perspective of a specialized pediatric neuro-oncological center describing the heterogeneous distribution of cases regarding age-related prevalence, tumor localization, and biology, which requires a high multidisciplinary expertise. The study contributes to define challenges in treating pediatric brain tumors and to develop quality indicators for pediatric neuro-oncological surgery. We assume that an adequate volume load of patients within a interdisciplinary infrastructure is warranted to aim for effective treatment and decent quality of life for the majority of long-term surviving pediatric tumor patients.
Keywords: Ependymoma; Extent of resection; High grade glioma; Medulloblastoma; Morbidity; Neurologic deficits; Pediatric brain tumor; Pilocytic Astrocytoma; Transfusion rates.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors have no financial or non-financial interests to disclose in relation to this study.
Figures


References
-
- Neervoort FW, Van Ouwerkerk WJ, Folkersma H, Kaspers GJ, Vandertop WP. Surgical morbidity and mortality of pediatric brain tumors: a single center audit. Child’s nervous system: ChNS: official journal of the International Society for Pediatric Neurosurgery. 2010;26:1583–1592. doi: 10.1007/s00381-010-1086-1. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
