

This is a preprint.
A Nanopore sequencing-based pharmacogenomic panel to personalize tuberculosis drug dosing
- PMID: 37732197
- PMCID: PMC10508808
- DOI: 10.1101/2023.09.08.23295248
A Nanopore sequencing-based pharmacogenomic panel to personalize tuberculosis drug dosing
Update in
-
A Nanopore Sequencing-based Pharmacogenomic Panel to Personalize Tuberculosis Drug Dosing.Am J Respir Crit Care Med. 2024 Jun 15;209(12):1486-1496. doi: 10.1164/rccm.202309-1583OC. Am J Respir Crit Care Med. 2024. PMID: 38647526 Free PMC article.
Abstract
Rationale: Standardized dosing of anti-tubercular (TB) drugs leads to variable plasma drug levels, which are associated with adverse drug reactions, delayed treatment response, and relapse. Mutations in genes affecting drug metabolism explain considerable interindividual pharmacokinetic variability; however, pharmacogenomic (PGx) assays that predict metabolism of anti-TB drugs have been lacking.
Objectives: To develop a Nanopore sequencing panel and validate its performance in active TB patients to personalize treatment dosing.
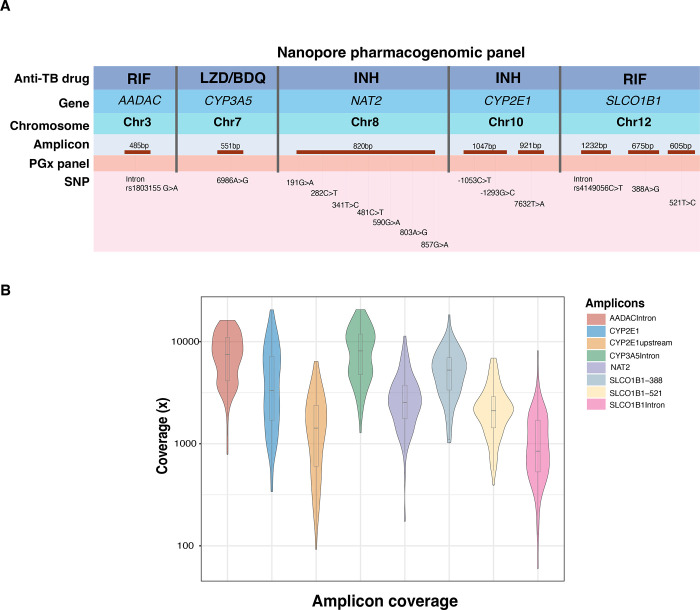
Measurements and main results: We developed a Nanopore sequencing panel targeting 15 single nucleotide polymorphisms (SNP) in 5 genes affecting the metabolism of isoniazid (INH), rifampin (RIF), linezolid and bedaquiline. For validation, we sequenced DNA samples (n=48) from the 1000 genomes project and compared variant calling accuracy with Illumina genome sequencing. We then sequenced DNA samples from patients with active TB (n=100) from South Africa on a MinION Mk1C and evaluated the relationship between genotypes and pharmacokinetic parameters for INH and RIF.
Results: The PGx panel achieved 100% concordance with Illumina sequencing in variant identification for the samples from the 1000 Genomes Project. In the clinical cohort, coverage was >100x for 1498/1500 (99.8%) amplicons across the 100 samples. One third (33%) of participants were identified as slow, 47% were intermediate and 20% were rapid isoniazid acetylators. Isoniazid clearance was significantly impacted by acetylator status (p<0.0001) with median (IQR) clearances of 11.2 L/h (9.3-13.4), 27.2 L/h (22.0-31.7), and 45.1 L/h (34.1-51.1) in slow, intermediate, and rapid acetylators. Rifampin clearance was 17.3% (2.50-29.9) lower in individuals with homozygous AADAC rs1803155 G>A substitutions (p=0.0015).
Conclusion: Targeted sequencing can enable detection of polymorphisms influencing TB drug metabolism on a low-cost, portable instrument to personalize dosing for TB treatment or prevention.
Keywords: NAT2; Nanopore; isoniazid; pharmacogenomics; targeted sequencing; tuberculosis.
Conflict of interest statement
Conflicts of Interest The authors declare no conflict of interest.
Figures



References
-
- Merle CS, Fielding K, Sow OB, Gninafon M, Lo MB, Mthiyane T, et al. OFLOTUB/Gatifloxacin for Tuberculosis Project. A four-month gatifloxacin-containing regimen for treating tuberculosis. N Engl J Med. 2014. Oct 23;371(17):1588–98. - PubMed
-
- Dorman SE, Nahid P, Kurbatova EV, Goldberg SV, Bozeman L, Burman WJ, et al. AIDS Clinical Trials Group and the Tuberculosis Trials Consortium. High-dose rifapentine with or without moxifloxacin for shortening treatment of pulmonary tuberculosis: Study protocol for TBTC study 31/ACTG A5349 phase 3 clinical trial. Contemp Clin Trials. 2020. Mar;90:105938. doi: 10.1016/j.cct.2020.105938. - DOI - PMC - PubMed
-
- Forget EJ, Menzies D. Adverse reactions to first-line antituberculosis drugs. Expert Opin Drug Saf. 2006. Mar;5(2):231–49. - PubMed
-
- Choi H, Park HA, Hyun IG, Kim JH, Hwang YI, Jang SH et al. Incidence and outcomes of adverse drug reactions to first-line anti-tuberculosis drugs and their effects on the quality of life: A multicenter prospective cohort study. Pharmacoepidemiol Drug Saf. 2022. Nov;31(11):1153–1163. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources