

This is a preprint.
Use of SGLT2i and ARNi in patients with atrial fibrillation and heart failure in 2021-2022: an analysis of real-world data
- PMID: 37732232
- PMCID: PMC10508822
- DOI: 10.1101/2023.09.08.23295280
Use of SGLT2i and ARNi in patients with atrial fibrillation and heart failure in 2021-2022: an analysis of real-world data
Update in
-
Use of Sodium-Glucose Cotransporter-2 Inhibitors and Angiotensin Receptor-Neprilysin Inhibitors in Patients With Atrial Fibrillation and Heart Failure From 2021 to 2022: An Analysis of Real-World Data.J Am Heart Assoc. 2024 Mar 19;13(6):e032783. doi: 10.1161/JAHA.123.032783. Epub 2024 Mar 8. J Am Heart Assoc. 2024. PMID: 38456406 Free PMC article.
Abstract
Objective: To evaluate utilization of sodium-glucose cotransporter-2 inhibitors (SGLT2i) and angiotensin receptor neprilysin inhibitors (ARNi) in patients with atrial fibrillation (AF) and heart failure (HF).
Methods: We analyzed the MarketScan databases for the period 1/1/2021 to 6/30/2022. Validated algorithms were used to identify patients with AF and HF, and to classify patients into HF with reduced ejection fraction (HFrEF) or preserved ejection fraction (HFpEF). We assessed the prevalence of SGLT2i and ARNi use overall and by HF type. Additionally, we explored correlates of lower utilization, including demographics and comorbidities.
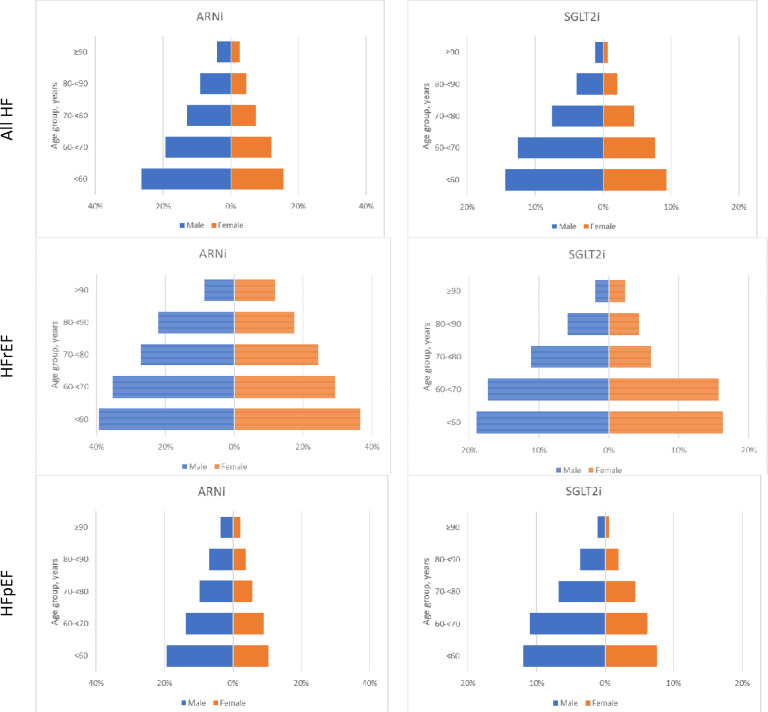
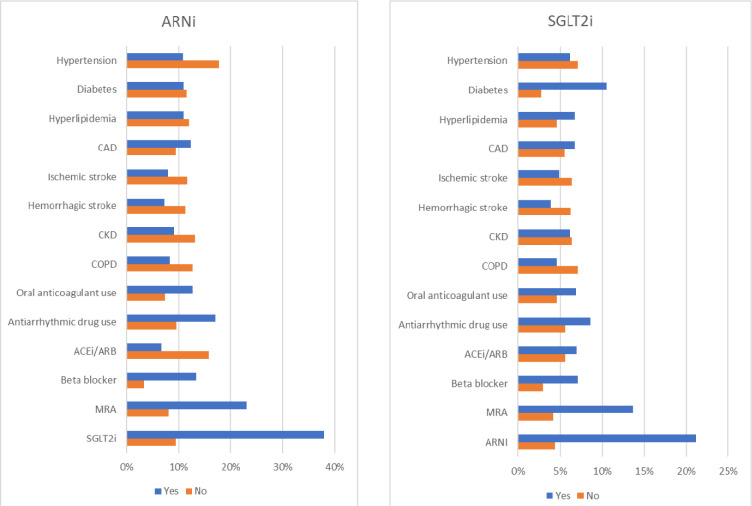
Results: The study population included 60,927 patients (mean age 75, 43% female) diagnosed with AF and HF (85% with HFpEF, 15% with HFrEF). Prevalence of ARNi use was 11% overall (30% in HFrEF, 8% in HFpEF), while the corresponding figure was 6% for SGLT2i (13% in HFrEF, 5% in HFpEF). Use of both medications increased over the study period: ARNi from 9% to 12% (from 22% to 29% in HFrEF, from 6% to 8% in HFpEF), and SGLT2i from 3% to 9% (from 6% to 16% in HFrEF, from 2% to 7% in HFpEF). Female sex, older age, and specific comorbidities were associated with lower utilization of these two medication types overall and by HF type.
Conclusion: Use of ARNi and SGLT2i in patients with AF and HF is suboptimal, particularly among females and older individuals, though utilization is increasing. These results underscore the need for understanding reasons for these disparities and developing interventions to improve adoption of evidence-based therapies among patients with comorbid AF and HF.
Figures

References
-
- Al-Khatib SM, Benjamin EJ, Albert CM, Alonso A, Chauhan C, Chen PS, Curtis AB, Desvigne-Nickens P, Ho JE, Lam CSP, et al. Advancing research on the complex interrelations between atrial fibrillation and heart failure: a report from a US National Heart, Lung, and Blood Institute virtual workshop. Circulation. 2020;141:1915–1926. - PMC - PubMed
-
- Cherian TS, Shrader P, Fonarow GC, Allen LA, Piccini JP, Peterson ED, Thomas L, Kowey PR, Gersh BJ, Mahaffey KW. Effect of atrial fibrillation on mortality, stroke risk, and quality-of-life scores in patients with heart failure (from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation [ORBIT-AF]). Am J Cardiol. 2017;119:1763–1769. - PubMed
-
- Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: epidemiology, pathophysiology, and rationale for therapy. Am J Cardiol. 2003;91:2d–8d. - PubMed
-
- Karnik AA, Gopal DM, Ko D, Benjamin EJ, Helm RH. Epidemiology of atrial fibrillation and heart failure: a growing and important problem. Cardiol Clin. 2019;37:119–129. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous