

Viral Detection by Reverse Transcriptase Polymerase Chain Reaction in Upper Respiratory Tract and Metagenomic RNA Sequencing in Lower Respiratory Tract in Critically Ill Children With Suspected Lower Respiratory Tract Infection
- PMID: 37732845
- PMCID: PMC10756702
- DOI: 10.1097/PCC.0000000000003336
Viral Detection by Reverse Transcriptase Polymerase Chain Reaction in Upper Respiratory Tract and Metagenomic RNA Sequencing in Lower Respiratory Tract in Critically Ill Children With Suspected Lower Respiratory Tract Infection
Abstract
Objectives: Viral lower respiratory tract infection (vLRTI) contributes to substantial morbidity and mortality in children. Diagnosis is typically confirmed by reverse transcriptase polymerase chain reaction (RT-PCR) of nasopharyngeal specimens in hospitalized patients; however, it is unknown whether nasopharyngeal detection accurately reflects presence of virus in the lower respiratory tract (LRT). This study evaluates agreement between viral detection from nasopharyngeal specimens by RT-PCR compared with metagenomic next-generation RNA sequencing (RNA-Seq) from tracheal aspirates (TAs).
Design: This is an analysis of of a seven-center prospective cohort study.
Setting: Seven PICUs within academic children's hospitals in the United States.
Patients: Critically ill children (from 1 mo to 18 yr) who required mechanical ventilation via endotracheal tube for greater than or equal to 72 hours.
Interventions: We evaluated agreement in viral detection between paired upper and LRT samples. Results of clinical nasopharyngeal RT-PCR were compared with TA RNA-Seq. Positive and negative predictive agreement and Cohen's Kappa were used to assess agreement.
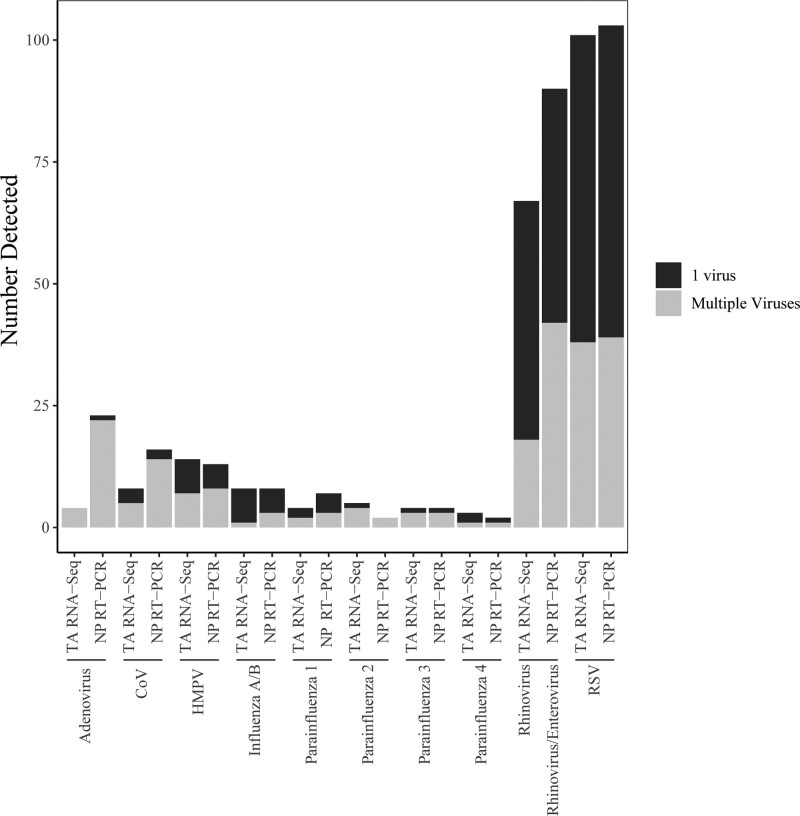
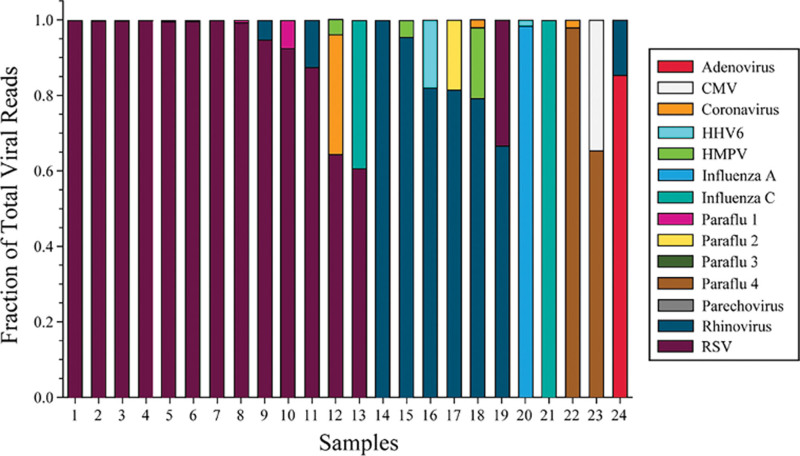
Measurements and main results: Of 295 subjects with paired testing available, 200 (68%) and 210 (71%) had positive viral testing by RT-PCR from nasopharyngeal and RNA-Seq from TA samples, respectively; 184 (62%) were positive by both nasopharyngeal RT-PCR and TA RNA-Seq for a virus, and 69 (23%) were negative by both methods. Nasopharyngeal RT-PCR detected the most abundant virus identified by RNA-Seq in 92.4% of subjects. Among the most frequent viruses detected, respiratory syncytial virus demonstrated the highest degree of concordance (κ = 0.89; 95% CI, 0.83-0.94), whereas rhinovirus/enterovirus demonstrated lower concordance (κ = 0.55; 95% CI, 0.44-0.66). Nasopharyngeal PCR was more likely to detect multiple viruses than TA RNA-Seq (54 [18.3%] vs 24 [8.1%], p ≤ 0.001).
Conclusions: Viral nucleic acid detection in the upper versus LRT reveals good overall agreement, but concordance depends on the virus. Further studies are indicated to determine the utility of LRT sampling or the use of RNA-Seq to determine LRTI etiology.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
This work was supported by the following cooperative agreements from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD): (UG1HD083171 to Dr. Pollack), (UG1HD049983 to Dr. Carcillo) (UG01HD049934 to Drs. Reeder, Locandro, and DeRisi), (UG1HD083170 to Dr. Hall), (UG1HD050096 to Dr. Meert), (UG1HD63108 to Dr. Zuppa), (UG1HD083166 to Dr. McQuillen), (UG1HD049981 to Dr. McQuillen); the National Heart Lung Blood Institute (1R01HL124103 to Dr. Pollack) and (K23HL138461-01A1 and 5R01HL155418-03 to Dr. Langelier), and National Institutes of Health (NIH). Dr. Maddux’s institution received funding from the National Institute for Child Health and Human Development (NICHD) (K23HD096018) and the Francis Family Foundation. Dr. Caldera disclosed work for hire and she disclosed that she is a staff research associate employed through University of California San Francisco. Dr. Hall received funding from Abbvie, Kiadis, and the American Board of Pediatrics. Drs. Zuppa, Carcillo, and McQuillen’s institutions received funding from the NICHD. Dr. Carcillo’s institution received funding from the National Institute of General Medical Sciences. Dr. DeRisi received funding from Public Health Company and Allen & Co; he disclosed that he is a scientific founder and advisor for Delve Bio; he received support for article research from Chan Zuckerberg Biohub. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Shi T, McAllister DA, O’Brien KL, et al. ; RSV Global Epidemiology Network: Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: A systematic review and modelling study. Lancet. 2017; 390:946–958 - PMC - PubMed
-
- Esposito S, Principi N: Defining the aetiology of paediatric community-acquired pneumonia: An unsolved problem. Expert Rev Respir Med. 2019; 13:153–161 - PubMed
MeSH terms
Grants and funding
- UG1 HD049983/HD/NICHD NIH HHS/United States
- UG1 HD063108/HD/NICHD NIH HHS/United States
- R01 HL155418/HL/NHLBI NIH HHS/United States
- K23 HL138461/HL/NHLBI NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- K23 HD096018/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- UG1 HD083170/HD/NICHD NIH HHS/United States
- UG1 HD083166/HD/NICHD NIH HHS/United States
- R01 HL124103/HL/NHLBI NIH HHS/United States
- UG1 HD083171/HD/NICHD NIH HHS/United States
- PL1 HD105462/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
