

Extended duration of treatment using reduced-frequency dosing of anti-PD-1 therapy in patients with advanced melanoma and Merkel cell carcinoma
- PMID: 37733060
- PMCID: PMC10576731
- DOI: 10.1007/s00262-023-03539-8
Extended duration of treatment using reduced-frequency dosing of anti-PD-1 therapy in patients with advanced melanoma and Merkel cell carcinoma
Erratum in
-
Correction to: Extended duration of treatment using reduced‑frequency dosing of anti‑PD‑1 therapy in patients with advanced melanoma and Merkel cell carcinoma.Cancer Immunol Immunother. 2023 Dec;72(12):4471. doi: 10.1007/s00262-023-03575-4. Cancer Immunol Immunother. 2023. PMID: 37979010 Free PMC article. No abstract available.
Abstract
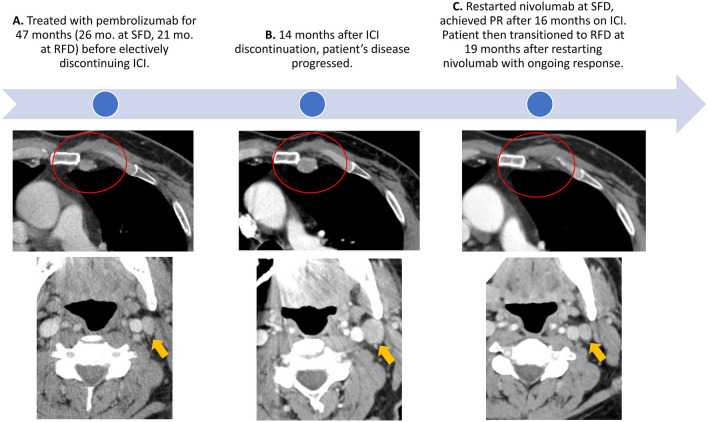
Background: Optimal duration of treatment (DoT) with immune checkpoint inhibitors (ICI) in metastatic cancers remains unclear. Many patients, especially those without radiologic complete remission, develop progressive disease after ICI discontinuation. Extending DoT with ICI may potentially improve efficacy outcomes but presents major logistical and cost challenges with standard frequency dosing (SFD). Receptor occupancy data supports reduced frequency dosing (RFD) of anti-PD-1 antibodies, which may represent a more practical and economically viable option to extend DoT.
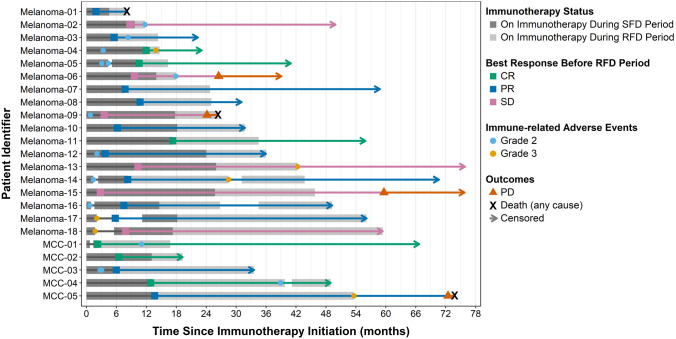
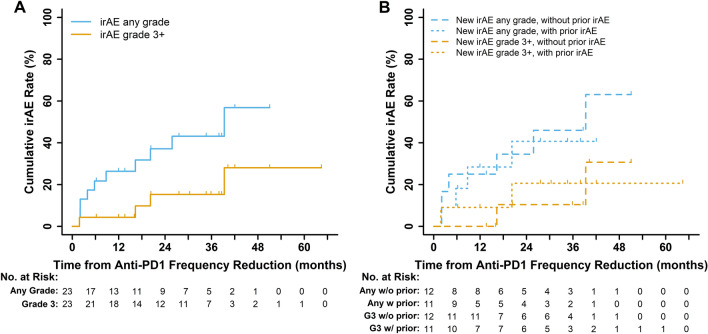
Methods: We conducted a retrospective study of patients with metastatic melanoma and Merkel cell carcinoma (MCC), who received ICI at RFD administered every 3 months, after initial disease control at SFD. We evaluated efficacy, safety, and cost-savings of the RFD approach in this cohort.
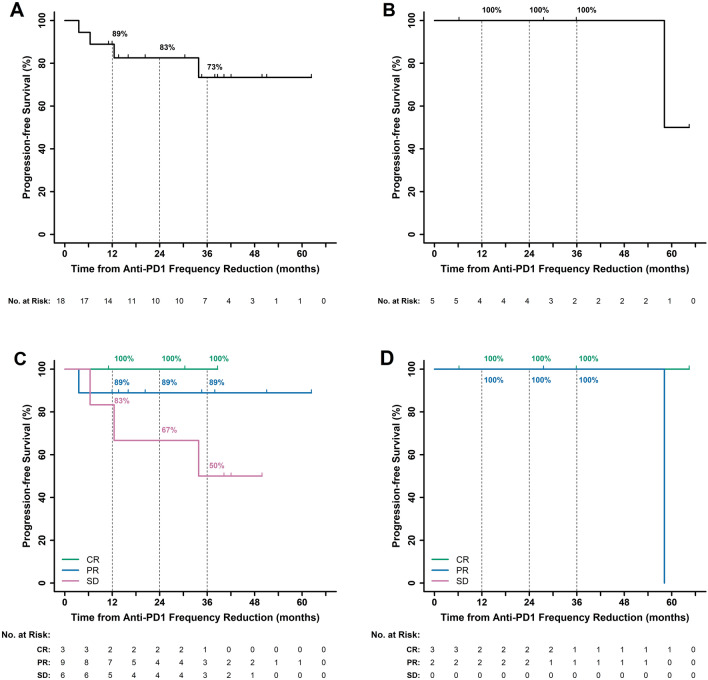
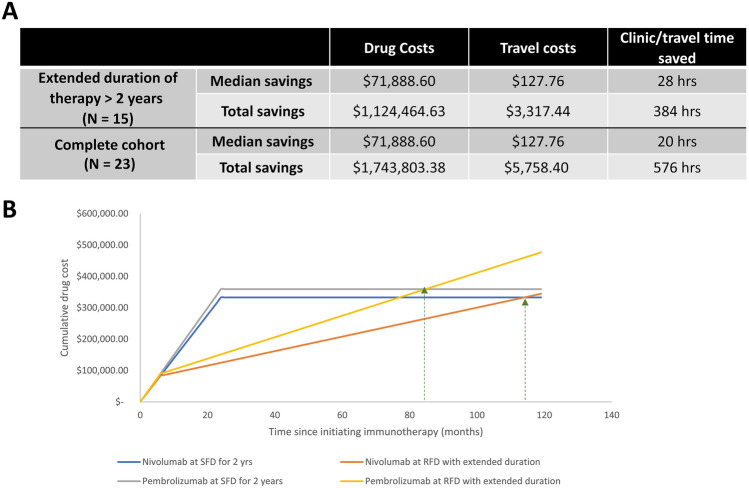
Results: Between 2014 and 2021, 23 patients with advanced melanoma (N = 18) or MCC (N = 5) received anti-PD-1 therapy at RFD. Median DoT was 1.1 years at SFD and 1.2 years at RFD. The 3 year PFS after start of RFD was 73% in melanoma and 100% in MCC patients, which compare favorably to historical control rates. In the subset of 15 patients who received at least 2 years of therapy, total savings amounted to $1.1 million in drug costs and 384 h saved despite the extended DoT (median 3.4 years), as compared to the calculated cost of 2 years at SFD.
Conclusions: ICI administration at RFD can allow extension of treatment duration, while preserving efficacy and reducing logistical and financial burden. RFD approach deserves further exploration in prospective clinical trials.
Keywords: Drug costs; Immunotherapy; Melanoma; Merkel cell carcinoma; Nivolumab; Pembrolizumab.
© 2023. The Author(s).
Conflict of interest statement
LT reports research grant funding (to institution) from Seagen and Merck; travel support from ASCO Merit Award. DH reports research grant funding from GE Healthcare. EH reports research grant funding (to institution) from Treatment Technologies and Insights, Neoleukin Technologies, ImCheck Therapeutics, Nektar, Replimune, and Nikang Therapeutics. JT reports consulting roles from Alpine, Bristol-Myer Squibb, and Mabquest; research grants (to institution) from Pfizer, Agensys, Five Prime Therapeutics, Trillium Therapeutics, Novarits, Xencor, Incyte, and PMV Pharma. JV reports stock and ownership, funding and intellectual property licensed to Lyell Immunopharma. DG reports stock and ownership interests in TailorMed and Vivio Health; consulting or advisory roles in Vivio Health; funding from MSD, BMS, and Janssen. PN reports consulting roles at 4SC, EMD Serono, Merck Sharp & Dohme, Pfizer, Pfizer/EMD Serono, and Sanofi/Regeneron; research grant funding from Bristol-Meyer Squibb and EMD Serono; patent filed for "Merkel cell polyomavirus T antigen-specific TCRs and uses thereof" and patent pending for high affinity T cell receptors that target the Merkel polyomavirus; travel expenses from Merck Sharp & Dohme and Sanofi/Regeneron. SB reports Advisory Board/Consultant (with honorarium) for Bristol Myers Squibb, Castle biosciences, EMD Serono, Exicure, Genentech, Sanofi-Genzyme and Incyte; Research Grants (to institution) from 4SC, Amphiyena Therapeutics, Bristol Myers Squibb, Checkmate, EMD Serono, Exicure, Immune Design, Incyte, Merck, NantKwest, Nektar, Novartis, OncoSec, Regeneron, Xencor; Stock/Equity in Moderna.
Figures
References
-
- Kaufman HL, Russell J, Hamid O, Bhatia S, Terheyden P, D'Angelo SP, et al. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: a multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. 2016;17(10):1374–1385. doi: 10.1016/S1470-2045(16)30364-3. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
