

Clinical validation of an AI-based automatic quantification tool for lung lobes in SPECT/CT
- PMID: 37733103
- PMCID: PMC10513978
- DOI: 10.1186/s40658-023-00578-z
Clinical validation of an AI-based automatic quantification tool for lung lobes in SPECT/CT
Abstract
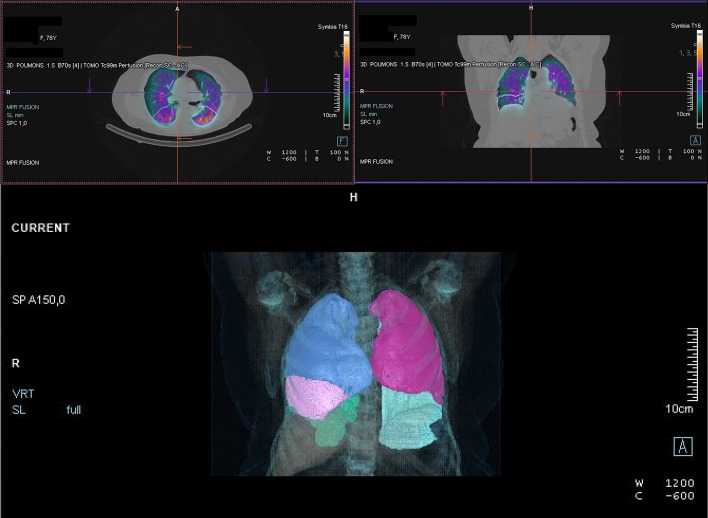
Background: Lung lobar ventilation and perfusion (V/Q) quantification is generally obtained by generating planar scintigraphy images and then imposing three equally sized regions of interest on the data of each lung. This method is fast but not as accurate as SPECT/CT imaging, which provides three-dimensional data and therefore allows more precise lobar quantification. However, the manual delineation of each lobe is time-consuming, which makes SPECT/CT incompatible with the clinical workflow for V/Q estimation. An alternative may be to use artificial intelligence-based auto-segmentation tools such as AutoLung3D (Siemens Healthineers, Knoxville, USA), which automatically delineate the lung lobes on the CT data acquired with the SPECT data. The present study assessed the clinical validity of this approach relative to planar scintigraphy and manual quantification in SPECT/CT.
Methods: The Autolung3D software was tested on the retrospective SPECT/CT data of 43 patients who underwent V/Q scintigraphy with 99mTc-macroaggregated albumin and 99mTc-labeled aerosol. It was compared to planar scintigraphy and SPECT/CT using the manual quantification method in terms of relative lobar V/Q quantification values and interobserver variability.
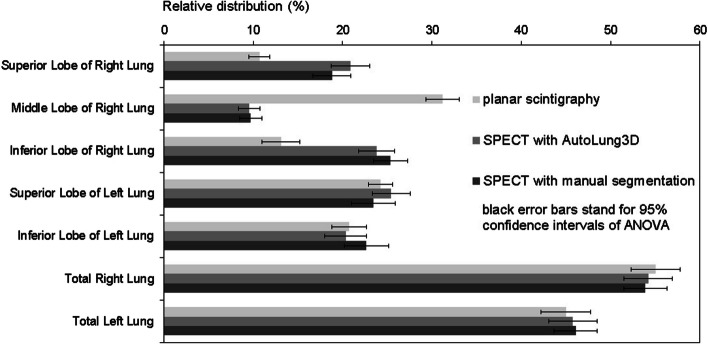
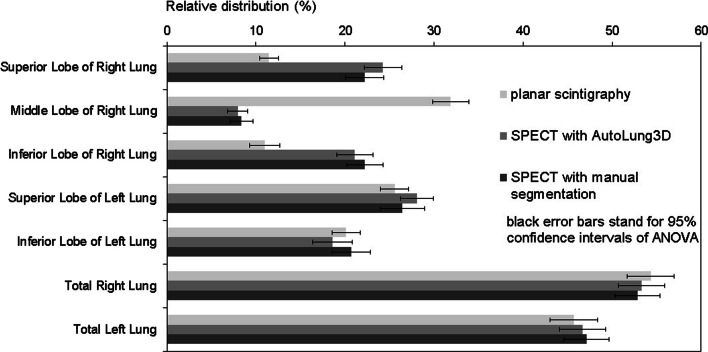
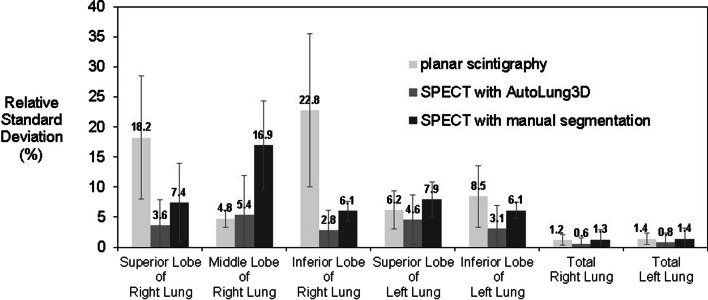
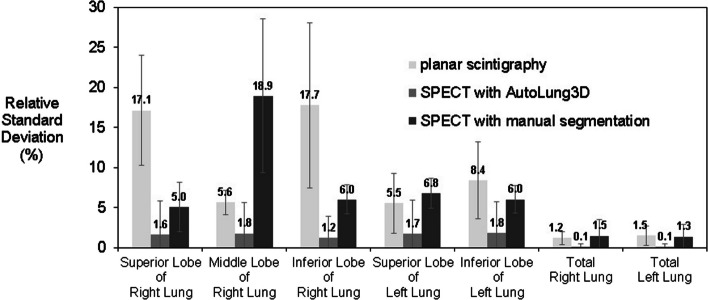
Results: The three methods provided similar V/Q estimates for the left lung lobes and total lungs. However, compared to the manual SPECT/CT method, planar scintigraphy yielded significantly higher estimates for the middle right lobe and significantly lower estimates for the superior and inferior right lobes. The estimates of the manual and automated SPECT/CT methods were similar. However, the post-processing time in the automated method was approximately 5 min compared to 2 h for the manual method. Moreover, the automated method associated with a drastic reduction in interobserver variability: Its maximal relative standard deviation was only 5%, compared to 23% for planar scintigraphy and 19% for the manual SPECT/CT method.
Conclusions: This study validated the AutoLung3D software for general clinical use since it rapidly provides accurate lobar quantification in V/Q scans with markedly less interobserver variability than planar scintigraphy or the manual SPECT/CT method.
Keywords: AI-based segmentation; Lobar quantification; Perfusion SPECT/CT; Ventilation SPECT/CT.
© 2023. Springer Nature Switzerland AG.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Brunelli A, Kim AW, Berger KI, Addrizzo-Harris DJ. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery. Chest. 2013;143(5)(Suppl):166–90 - PubMed
LinkOut - more resources
Full Text Sources
