

Paradigm Shift: Multiple Potential Pathways to Neurodegenerative Dementia
- PMID: 37733209
- PMCID: PMC10684852
- DOI: 10.1007/s13311-023-01441-w
Paradigm Shift: Multiple Potential Pathways to Neurodegenerative Dementia
Abstract
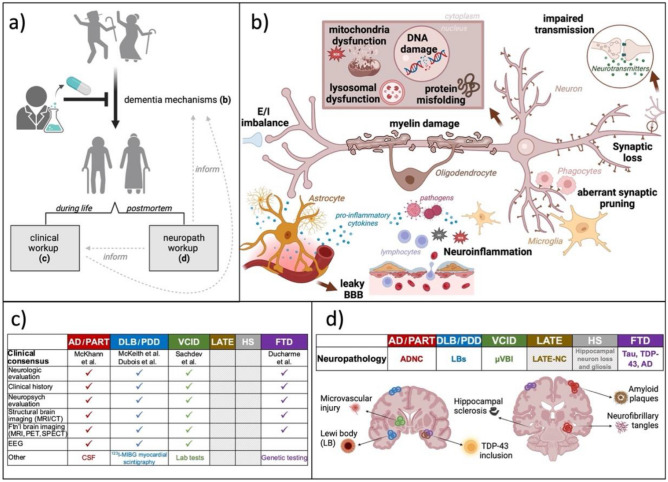
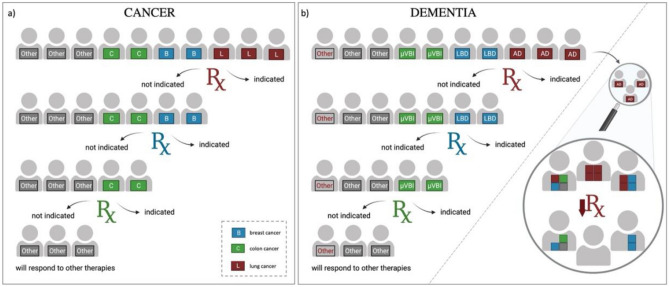
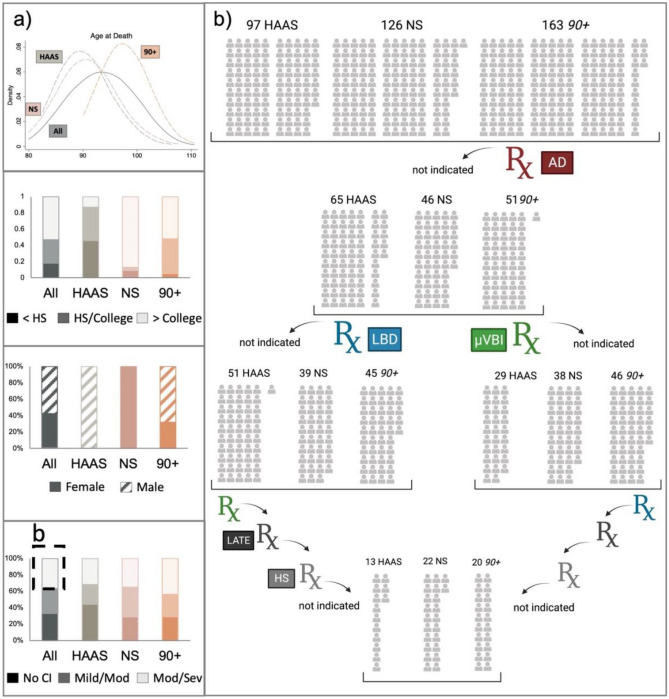
Neurodegenerative dementia can result from multiple underlying abnormalities, including neurotransmitter imbalances, protein aggregation, and other neurotoxic events. A major complication in identifying effective treatment targets is the frequent co-occurrence of multiple neurodegenerative processes, occurring either in parallel or sequentially. The path towards developing effective treatments for Alzheimer's disease (AD) and other dementias has been relatively slow and until recently has focused on disease symptoms. Aducanumab and lecanemab, recently approved by the FDA, are meant to target disease structures but have only modest benefit on symptom progression and remain unproven in reversing or preventing dementia. A third, donanemab, appears more promising but awaits FDA approval. Ongoing trials include potential cognition enhancers, new combinations of known drugs for synergistic effects, prodrugs with less toxicity, and increasing interest in drugs targeting neuroinflammation or microbiome. Scientific and technological advances offer the opportunity to move in new therapy directions, such as modifying microglia to prevent or suppress underlying disease. A major challenge, however, is that underlying comorbidities likely influence the effectiveness of therapies. Indeed, the full range of comorbidity, today only definitively identified postmortem, likely contributes to failed clinical trials and overmedication of older adults, since it is difficult to exclude (during life) people unlikely to respond. Our current knowledge thus signals that a paradigm shift towards individualized and multimodal treatments is necessary to effectively advance the field of dementia therapeutics.
Keywords: Alzheimer’s disease; Dementia; Lewy body disease; Microglia; Neuropathologic comorbidity.
© 2023. The American Society for Experimental Neurotherapeutics, Inc.
Conflict of interest statement
All authors have no conflict of interest.
Figures
Similar articles
-
[Anti-amyloid Antibody Drugs as Disease-Modifying Therapies for Alzheimer's Disease].Brain Nerve. 2024 Sep;76(9):991-995. doi: 10.11477/mf.1416202723. Brain Nerve. 2024. PMID: 39251217 Review. Japanese.
-
How promising are the latest monoclonal antibodies targeting amyloid-β for the treatment of early Alzheimer's disease?Expert Opin Emerg Drugs. 2024 Mar;29(1):35-43. doi: 10.1080/14728214.2024.2304059. Epub 2024 Jan 12. Expert Opin Emerg Drugs. 2024. PMID: 38193477 Review.
-
Guidelines for pharmacotherapy in Alzheimer's disease - A primer on FDA-approved drugs.J Neurosci Rural Pract. 2023 Oct-Dec;14(4):566-573. doi: 10.25259/JNRP_356_2023. Epub 2023 Oct 7. J Neurosci Rural Pract. 2023. PMID: 38059250 Free PMC article. Review.
-
Pharmacokinetic evaluation of donanemab for the treatment of Alzheimer's.Expert Opin Drug Metab Toxicol. 2024 Jun;20(6):411-417. doi: 10.1080/17425255.2024.2357637. Epub 2024 May 20. Expert Opin Drug Metab Toxicol. 2024. PMID: 38758223 Review.
-
Profiling lecanemab as a treatment option for Alzheimer's disease.Expert Rev Neurother. 2024 May;24(5):433-441. doi: 10.1080/14737175.2024.2333970. Epub 2024 Apr 3. Expert Rev Neurother. 2024. PMID: 38566584 Review.
Cited by
-
Prevention and Treatment of Alzheimer's Disease Via the Regulation of the Gut Microbiota With Traditional Chinese Medicine.CNS Neurosci Ther. 2024 Nov;30(11):e70101. doi: 10.1111/cns.70101. CNS Neurosci Ther. 2024. PMID: 39508315 Free PMC article. Review.
-
Beyond the usual suspects: multi-factorial computational models in the search for neurodegenerative disease mechanisms.Transl Psychiatry. 2024 Sep 23;14(1):386. doi: 10.1038/s41398-024-03073-w. Transl Psychiatry. 2024. PMID: 39313512 Free PMC article. Review.
References
-
- McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7:263–269. doi: 10.1016/j.jalz.2011.03.005. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
