

The Significance of Hematuria in Podocytopathies
- PMID: 37733352
- PMCID: PMC10843204
- DOI: 10.2215/CJN.0000000000000309
The Significance of Hematuria in Podocytopathies
Abstract
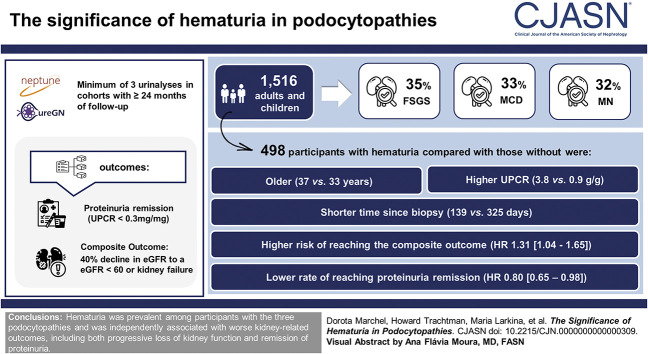
Background: Hematuria is frequently present in podocytopathies, but its significance and prognostic value is not well described in these proteinuric kidney diseases. This study describes the prevalence and association between hematuria and kidney-related outcomes in these disorders.
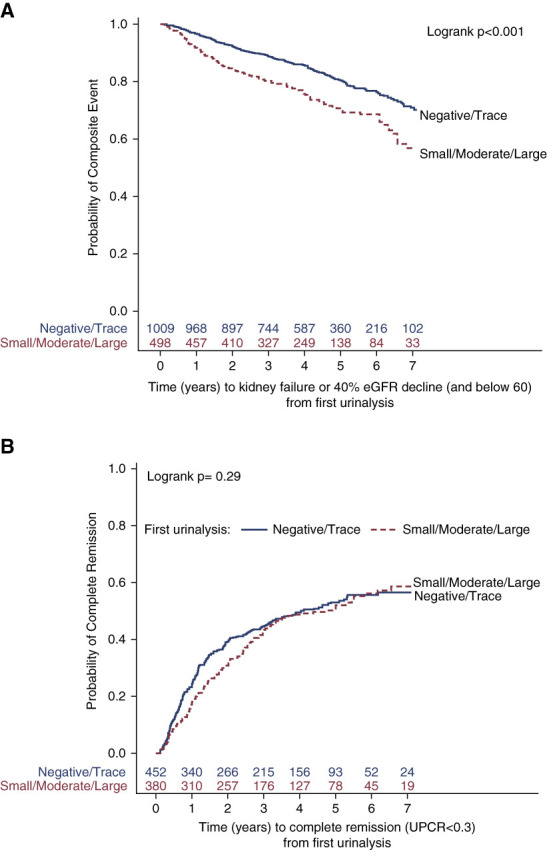
Methods: Hematuria was assessed at the initial urinalysis in participants with the following podocytopathies-membranous nephropathy, minimal change disease, and FSGS-in the Nephrotic Syndrome Study Network and Cure Glomerulonephropathy cohorts with >24 months of follow-up. Multivariable Cox proportional hazards models were fit for time to composite outcome (kidney failure or 40% decline in eGFR and eGFR <60 ml/min per 1.73 m 2 ) and proteinuria remission (urine protein-to-creatinine ratio [UPCR] <0.3 mg/mg).
Results: Among the 1516 adults and children in the study, 528 participants (35%) had FSGS, 499 (33%) had minimal change disease, and 489 (32%) had membranous nephropathy. Median (interquartile range) time from biopsy until the initial study urinalysis was 260 (49-750) days, and 498 participants (33%) were positive for hematuria. Participants with hematuria compared with those without were older (37 [16-55] versus 33 [12-55] years), more likely to have an underlying diagnosis of membranous nephropathy (44% versus 27%), had shorter time since biopsy (139 [27-477] versus 325 [89-878] days), and had higher UPCR (3.8 [1.4-8.0] versus 0.9 [0.1-3.1] g/g). After adjusting for diagnosis, age, sex, UPCR, eGFR, time since biopsy, and study cohort, hematuria was associated with a higher risk of reaching the composite outcome (hazard ratio, 1.31; 95% confidence interval, 1.04 to 1.65; P value, 0.02) and lower rate of reaching proteinuria remission (hazard ratio, 0.80; 95% confidence interval, 0.65 to 0.98; P value, 0.03).
Conclusions: Hematuria is prevalent among participants with the three podocytopathies and is significantly and independently associated with worse kidney-related outcomes, including both progressive loss of kidney function and remission of proteinuria.
Copyright © 2023 by the American Society of Nephrology.
Conflict of interest statement
A.S. Bomback reports consultancy for Amgen, Apellis, Catalyst, Genentech, Kezar, Novartis, Q32, Silence Therapeutics, and Visterra and honoraria from Alexion, ANI, Aurinia, Calliditas, GlaxoSmithKline, Principio, Travere, and UpToDate. P.A. Canetta reports consultancy for Chinook, Novartis, Otsuka, and Travere and research funding from Calliditas, Novartis, and Travere. D. Fermin reports employment with University of Michigan and ownership interest in 10X Genomics, AstraZeneca, Moderna, and Thermo-Fisher Scientific. D.S. Gipson reports employment with NIH/NIDDK/KUH; consultancy between AstraZeneca, Boehringer-Ingelheim, Genentech (no individual consultancy agreements), Goldfinch Bio, Roche, University of Michigan, and Vertex; research funding to University of Michigan from Boehringer-Ingelheim, Genentech/Roche, Goldfinch Bio, Novartis, Reata, and Travere; role on advisory boards/steering committees for AstraZeneca, Goldfinch Bio, Roche/Genentech, and Vertex; member of the Kidney Health Initiative focal segmental glomerulosclerosis and Pediatric IgA Nephropathy projects; Editorial Board member of
Figures

References
MeSH terms
Grants and funding
- U24 DK100845/DK/NIDDK NIH HHS/United States
- U01DK100866/DK/NIDDK NIH HHS/United States
- U01 DK100867/DK/NIDDK NIH HHS/United States
- U01 DK100866/DK/NIDDK NIH HHS/United States
- U2C TR002818/TR/NCATS NIH HHS/United States
- U54 DK083912/DK/NIDDK NIH HHS/United States
- R01 DK119380/DK/NIDDK NIH HHS/United States
- U01 DK100876/DK/NIDDK NIH HHS/United States
- U24DK100845/DK/NIDDK NIH HHS/United States
- U01DK100867/DK/NIDDK NIH HHS/United States
- U2CTR002818/NS/NINDS NIH HHS/United States
- U01 DK100846/DK/NIDDK NIH HHS/United States
- U54DK083912/DK/NIDDK NIH HHS/United States
- K12 HD028820/HD/NICHD NIH HHS/United States
- U01DK100876/DK/NIDDK NIH HHS/United States
- U01DK100846/DK/NIDDK NIH HHS/United States
- UM1 DK100867/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
