

Germline Sequencing Analysis to Inform Clinical Gene Panel Testing for Aggressive Prostate Cancer
- PMID: 37733366
- PMCID: PMC10881219
- DOI: 10.1001/jamaoncol.2023.3482
Germline Sequencing Analysis to Inform Clinical Gene Panel Testing for Aggressive Prostate Cancer
Abstract
Importance: Germline gene panel testing is recommended for men with advanced prostate cancer (PCa) or a family history of cancer. While evidence is limited for some genes currently included in panel testing, gene panels are also likely to be incomplete and missing genes that influence PCa risk and aggressive disease.
Objective: To identify genes associated with aggressive PCa.
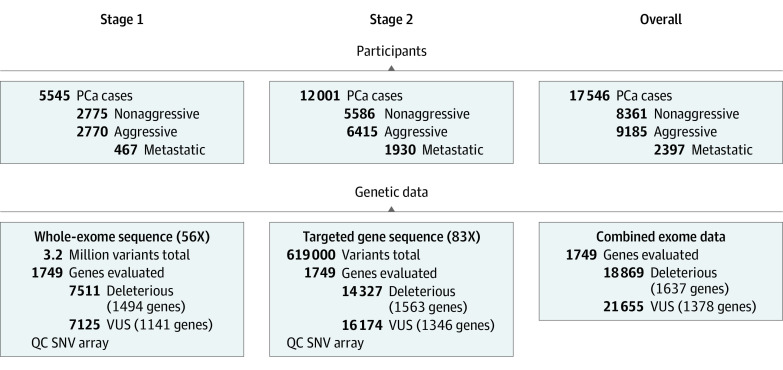
Design, setting, and participants: A 2-stage exome sequencing case-only genetic association study was conducted including men of European ancestry from 18 international studies. Data analysis was performed from January 2021 to March 2023. Participants were 9185 men with aggressive PCa (including 6033 who died of PCa and 2397 with confirmed metastasis) and 8361 men with nonaggressive PCa.
Exposure: Sequencing data were evaluated exome-wide and in a focused investigation of 29 DNA repair pathway and cancer susceptibility genes, many of which are included on gene panels.
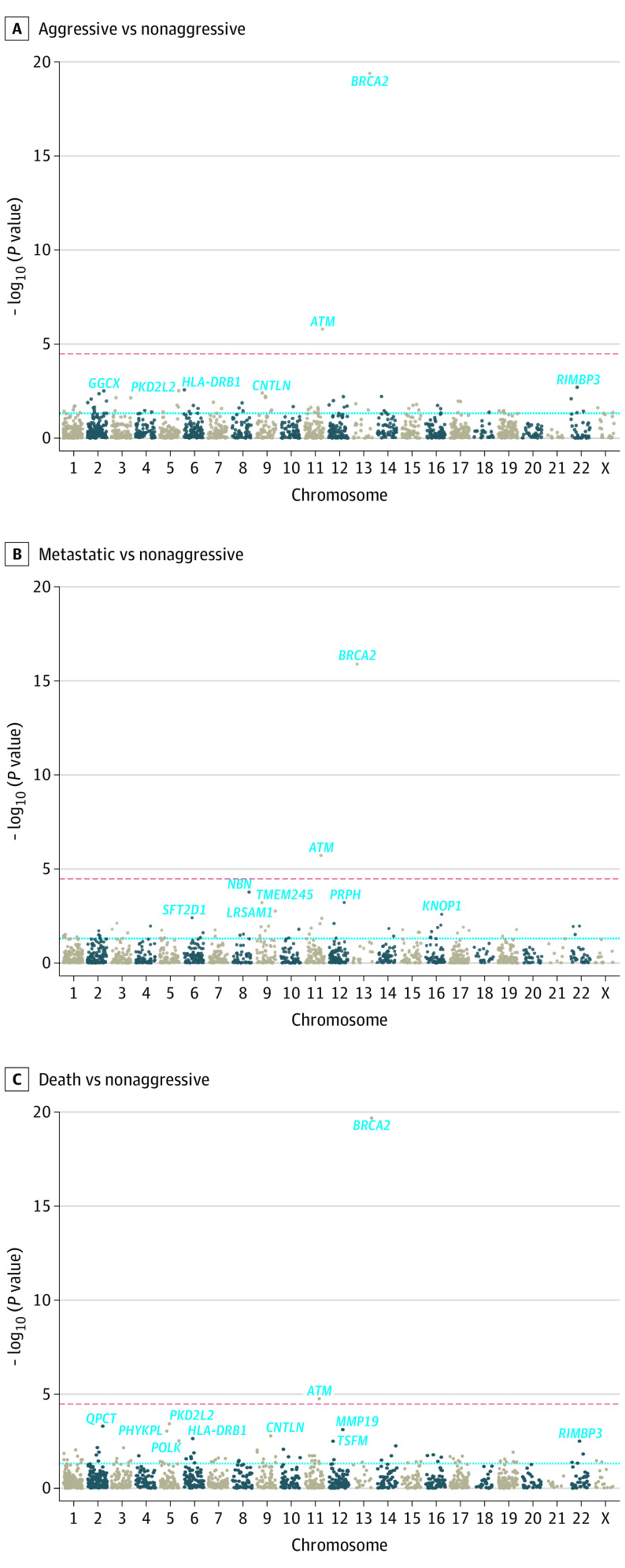
Main outcomes and measures: The primary study outcomes were aggressive (category T4 or both T3 and Gleason score ≥8 tumors, metastatic PCa, or PCa death) vs nonaggressive PCa (category T1 or T2 and Gleason score ≤6 tumors without known recurrence), and metastatic vs nonaggressive PCa.
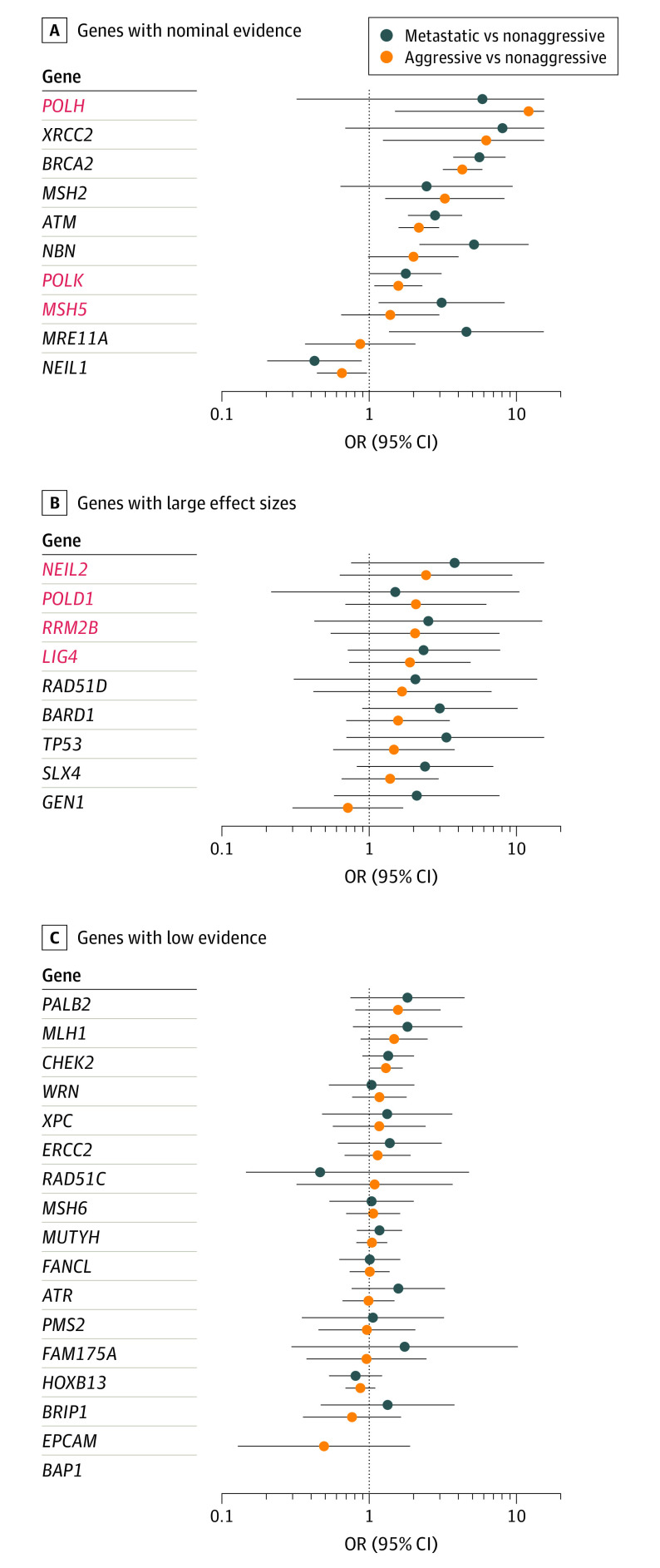
Results: A total of 17 546 men of European ancestry were included in the analyses; mean (SD) age at diagnosis was 65.1 (9.2) years in patients with aggressive PCa and 63.7 (8.0) years in those with nonaggressive disease. The strongest evidence of association with aggressive or metastatic PCa was noted for rare deleterious variants in known PCa risk genes BRCA2 and ATM (P ≤ 1.9 × 10-6), followed by NBN (P = 1.7 × 10-4). This study found nominal evidence (P < .05) of association with rare deleterious variants in MSH2, XRCC2, and MRE11A. Five other genes had evidence of greater risk (OR≥2) but carrier frequency differences between aggressive and nonaggressive PCa were not statistically significant: TP53, RAD51D, BARD1, GEN1, and SLX4. Deleterious variants in these 11 candidate genes were carried by 2.3% of patients with nonaggressive, 5.6% with aggressive, and 7.0% with metastatic PCa.
Conclusions and relevance: The findings of this study provide further support for DNA repair and cancer susceptibility genes to better inform disease management in men with PCa and for extending testing to men with nonaggressive disease, as men carrying deleterious alleles in these genes are likely to develop more advanced disease.
Conflict of interest statement
Figures
Comment in
-
Rare Genetic Drivers of Lethal Prostate Cancer.JAMA Oncol. 2023 Nov 1;9(11):1499-1501. doi: 10.1001/jamaoncol.2023.3352. JAMA Oncol. 2023. PMID: 37733349 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
