

Suboptimal gestational weight gain and neonatal outcomes in low and middle income countries: individual participant data meta-analysis
- PMID: 37734757
- PMCID: PMC10512803
- DOI: 10.1136/bmj-2022-072249
Suboptimal gestational weight gain and neonatal outcomes in low and middle income countries: individual participant data meta-analysis
Abstract
Objective: To estimate the associations between gestational weight gain (GWG) during pregnancy and neonatal outcomes in low and middle income countries.
Design: Individual participant data meta-analysis.
Setting: Prospective pregnancy studies from 24 low and middle income countries.
Main outcome measures: Nine neonatal outcomes related to timing (preterm birth) and anthropometry (weight, length, and head circumference) at birth, stillbirths, and neonatal death.
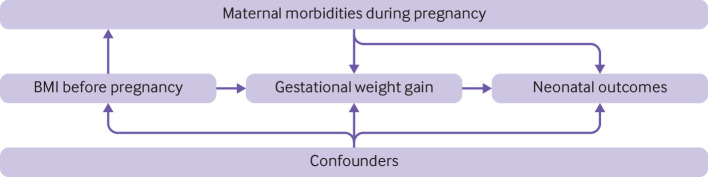
Analysis methods: A systematic search was conducted in PubMed, Embase, and Web of Science which identified 53 prospective pregnancy studies published after the year 2000 with data on GWG, timing and anthropometry at birth, and neonatal mortality. GWG adequacy was defined as the ratio of the observed maternal weight gain over the recommended weight gain based on the Institute of Medicine body mass index specific guidelines, which are derived from data in high income settings, and the INTERGROWTH-21st GWG standards. Study specific estimates, adjusted for confounders, were generated and then pooled using random effects meta-analysis models. Maternal age and body mass index before pregnancy were examined as potential modifiers of the associations between GWG adequacy and neonatal outcomes.
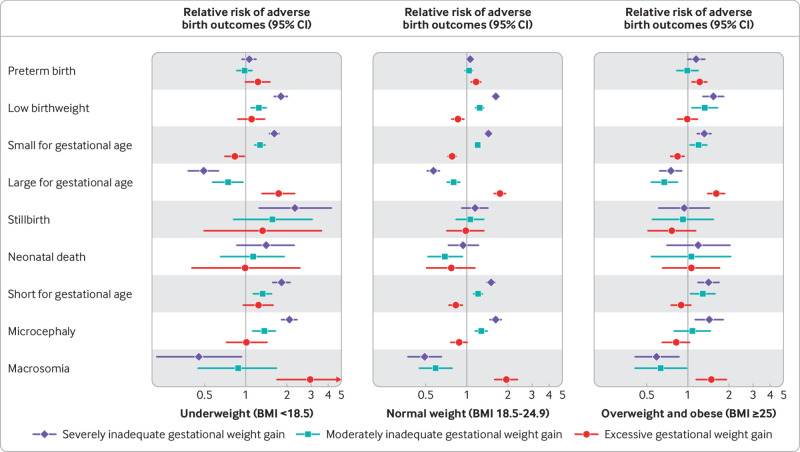
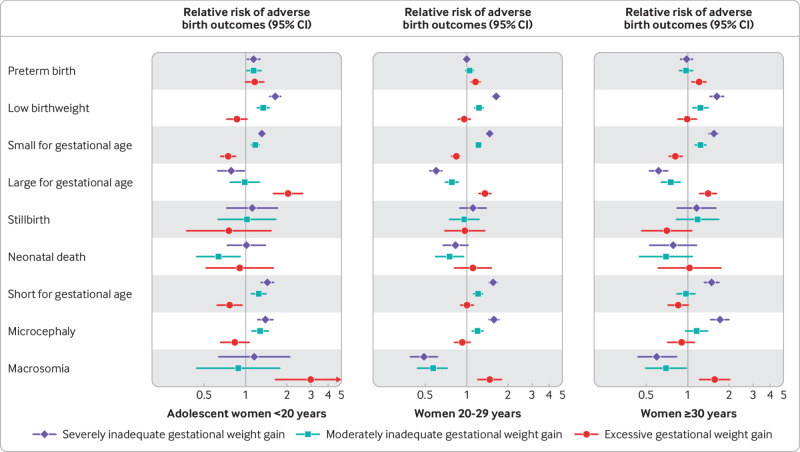
Results: Overall, 55% of participants had severely inadequate (<70%) or moderately inadequate (70% to <90%) GWG, 22% had adequate GWG (90-125%), and 23% had excessive GWG (≥125%). Severely inadequate GWG was associated with a higher risk of low birthweight (adjusted relative risk 1.62, 95% confidence interval 1.51 to 1.72; 48 studies, 93 337 participants; τ2=0.006), small for gestational age (1.44, 1.36 to 1.54; 51 studies, 93 191 participants; τ2=0.016), short for gestational age (1.47, 1.29 to 1.69; 40 studies, 83 827 participants; τ2=0.074), and microcephaly (1.57, 1.31 to 1.88; 31 studies, 80 046 participants; τ2=0.145) compared with adequate GWG. Excessive GWG was associated with a higher risk of preterm birth (1.22, 1.13 to 1.31; 48 studies, 103 762 participants; τ2=0.008), large for gestational age (1.44, 1.33 to 1.57; 47 studies, 90 044 participants; τ2=0.009), and macrosomia (1.52, 1.33 to 1.73; 29 studies, 68 138 participants; τ2=0) compared with adequate GWG. The direction and magnitude of the associations between GWG adequacy and several neonatal outcomes were modified by maternal age and body mass index before pregnancy.
Conclusions: Inadequate and excessive GWG are associated with a higher risk of adverse neonatal outcomes across settings. Interventions to promote optimal GWG during pregnancy are likely to reduce the burden of adverse neonatal outcomes, however further research is needed to assess optimal ranges of GWG based on data from low and middle income countries.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: financial support for the submitted work from the Bill and Melinda Gates Foundation, the Canadian Institutes of Health Research, the National Institutes of Health, the European Union’s Seventh Framework Programme and the Spanish Government, the UK Medical Research Council and the Department for International Development (DFID) under the MRC/DFID Concordat agreement, the National Council for Scientific and Technological Development (CNPq), Maria Cecilia Souto Vidigal Foundation Brazil, São Paulo State Research Foundation (FAPESP), Fondo Nestlé-Funsalud, Coordination for the Improvement of Higher Education Personnel (CAPES) and the Wellcome Trust; financial support from the World Health Organization for performance of work for the project ‘Global gestational weight gain standards’ to GK and the Family Larsson-Rosenquist Foundation to SHK; no other associations or activities that could appear to have influenced the submitted work.
Figures
References
-
- Institute of Medicine, National Research Council. Weight Gain during Pregnancy: Reexamining the Guidelines (Rasmussen KM, Yaktine AL, eds.). The National Academies Press; 2009. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources