

Hypoxic burden to guide CPAP treatment allocation in patients with obstructive sleep apnoea: a post hoc study of the ISAACC trial
- PMID: 37734857
- PMCID: PMC10701092
- DOI: 10.1183/13993003.00828-2023
Hypoxic burden to guide CPAP treatment allocation in patients with obstructive sleep apnoea: a post hoc study of the ISAACC trial
Abstract
Background: Hypoxic burden (HB) has emerged as a strong predictor of cardiovascular risk in obstructive sleep apnoea (OSA). We aimed to assess the potential of HB to predict the cardiovascular benefit of treating OSA with continuous positive airway pressure (CPAP).
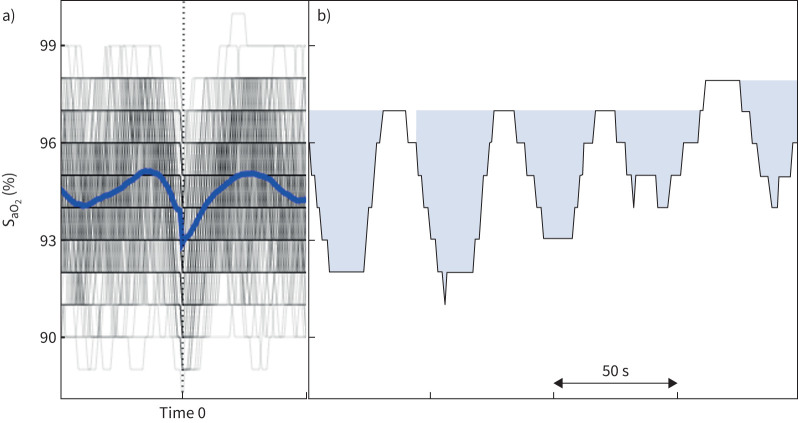
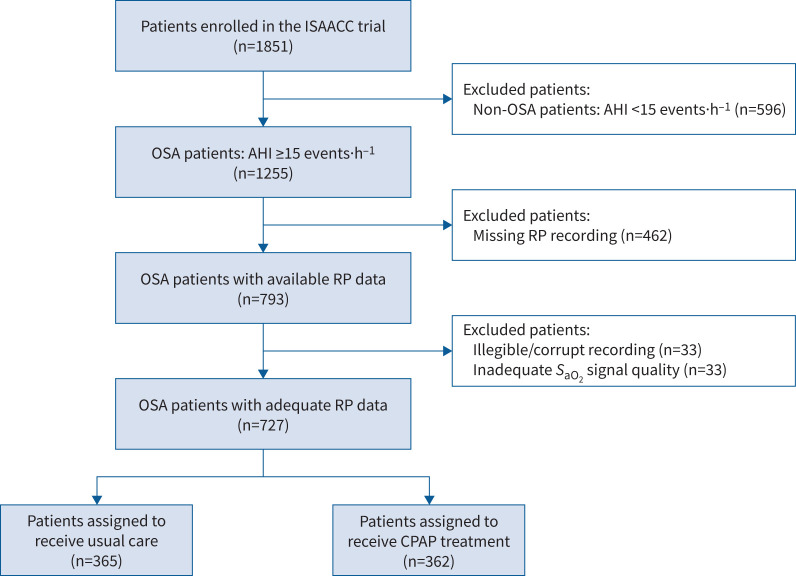
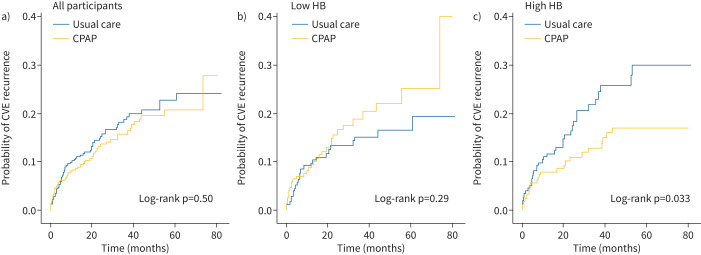
Methods: This was a post hoc analysis of the ISAACC trial (ClinicalTrials.gov: NCT01335087) including non-sleepy patients with acute coronary syndrome (ACS) diagnosed with OSA (apnoea-hypopnoea index ≥15 events·h-1) by respiratory polygraphy. Patients were randomised to CPAP or usual care and followed for a minimum of 1 year. HB was calculated as the total area under all automatically identified desaturations divided by total sleep time. Patients were categorised as having high or low baseline HB according to the median value (73.1%min·h-1). Multivariable Cox regression models were used to assess whether the effect of CPAP on the incidence of cardiovascular outcomes was dependent on the baseline HB level.
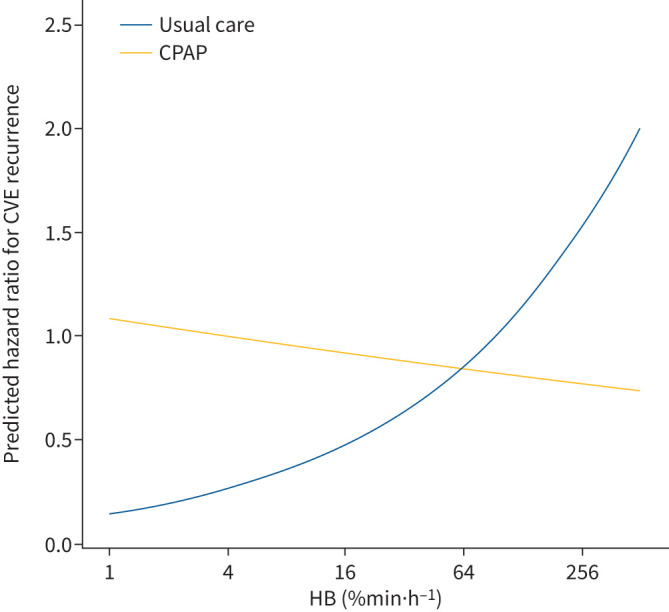
Results: The population (362 patients assigned to CPAP and 365 patients assigned to usual care) was middle-aged (mean age 59.7 years), overweight/obese and mostly male (84.5%). A significant interaction was found between the treatment arm and the HB categories. In the high HB group, CPAP treatment was associated with a significant reduction in the incidence of cardiovascular events (HR 0.57, 95% CI 0.34-0.96). In the low HB group, CPAP-treated patients exhibited a trend toward a higher risk of cardiovascular outcomes than those receiving usual care (HR 1.33, 95% CI 0.79-2.25). The differential effect of the treatment depending on the baseline HB level followed a dose-response relationship.
Conclusion: In non-sleepy ACS patients with OSA, high HB levels were associated with a long-term protective effect of CPAP on cardiovascular prognosis.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: M.Á. Martinez-Garcia received grants from VitalAire and Philips, Spain, and serves as a consultant for ResMed Inc., Australia, companies that develop products related to sleep apnoea. L. Messineo received a consultancy fee from Apnimed. A. Wellman works as a consultant for Apnimed, SomniFix and Nox, and has received grants from SomniFix and Sanofi; A. Wellman has a financial interest in Apnimed, a company developing pharmacological therapies for sleep apnoea. His interests were reviewed and are managed by Brigham and Women's Hospital and Partners HealthCare in accordance with their conflict of interest policies. S. Redline received grant support and consulting fees from Jazz Pharmaceuticals, and consulting fees from Apnimed and Lilly Pharma. S. Sands receives personal fees as a consultant for Nox Medical and Merck, outside the submitted work, and receives grant support from Apnimed and ProSomnus. F. Barbé received a research grant from ResMed Inc., Australia, a company that develops products related to sleep apnoea. A. Azarbarzin reports grant support from SomniFix and serves as a consultant for SomniFix, Respicardia, Eli Lilly and Apnimed. Apnimed is developing pharmacological treatments for obstructive sleep apnoea. A. Azarbarzin's interests were reviewed by Brigham and Women's Hospital and Mass General Brigham in accordance with their institutional policies. All other authors declare no competing interests.
Figures
Comment in
-
Continuous positive airway pressure for prevention of cardiovascular events and mortality: why evidence is evolving.Eur Respir J. 2023 Dec 7;62(6):2301741. doi: 10.1183/13993003.01741-2023. Print 2023 Dec. Eur Respir J. 2023. PMID: 38061793 No abstract available.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical