

Automatic analysis of bronchus-artery dimensions to diagnose and monitor airways disease in cystic fibrosis
- PMID: 37734952
- PMCID: PMC10803964
- DOI: 10.1136/thorax-2023-220021
Automatic analysis of bronchus-artery dimensions to diagnose and monitor airways disease in cystic fibrosis
Abstract
Background: Cystic fibrosis (CF) lung disease is characterised by progressive airway wall thickening and widening. We aimed to validate an artificial intelligence-based algorithm to assess dimensions of all visible bronchus-artery (BA) pairs on chest CT scans from patients with CF.
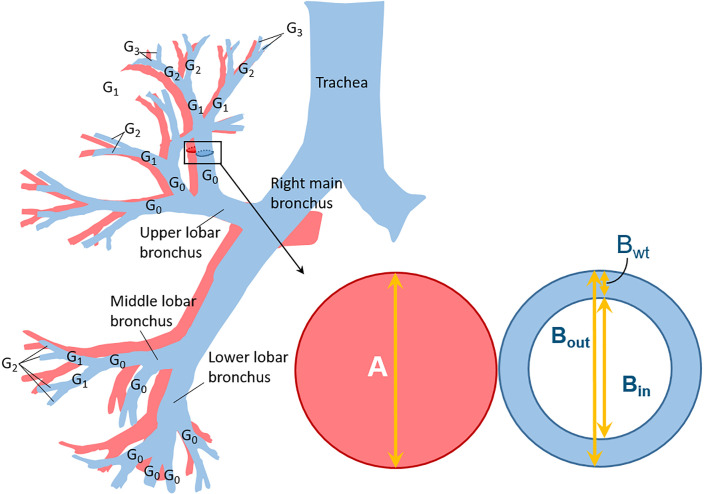
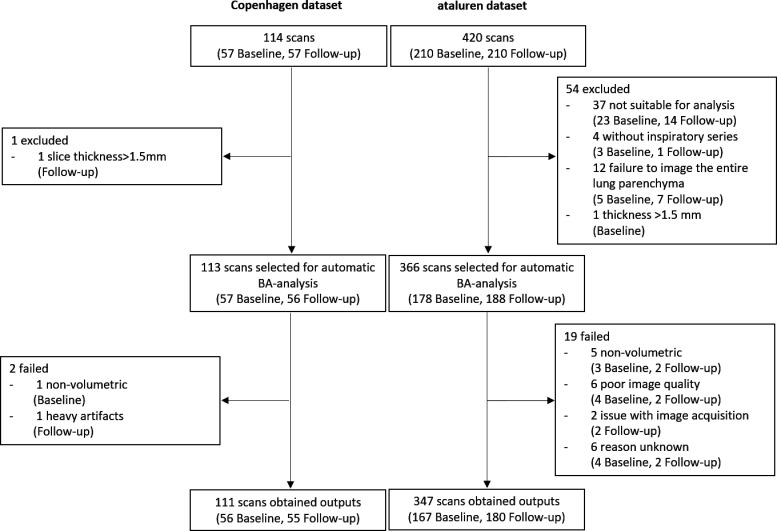
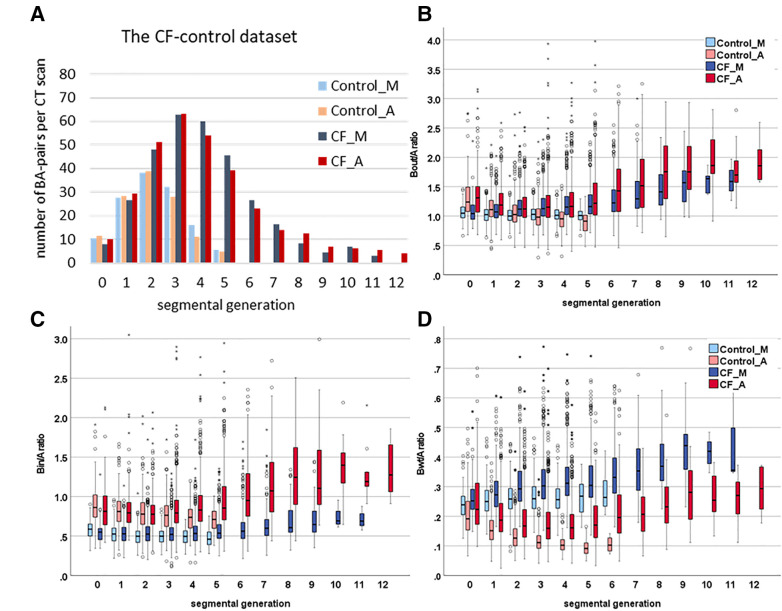
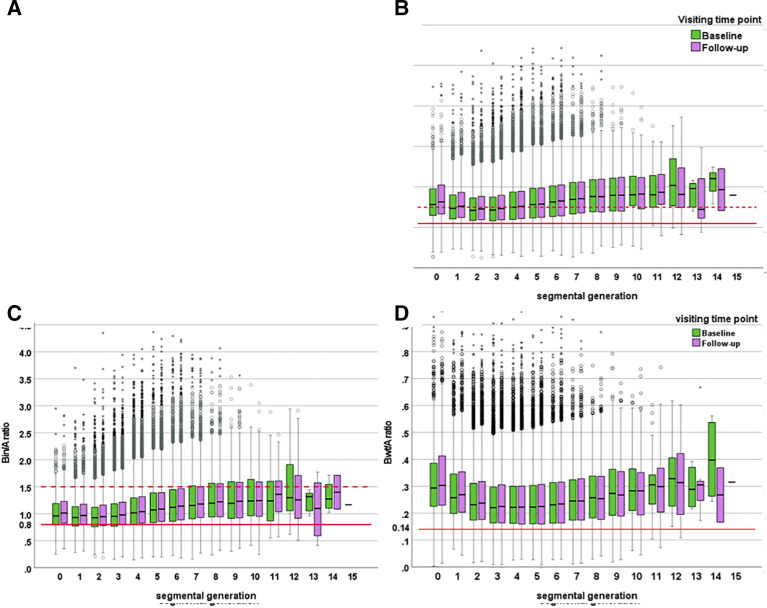
Methods: The algorithm fully automatically segments the bronchial tree; identifies bronchial generations; matches bronchi with the adjacent arteries; measures for each BA-pair bronchial outer diameter (Bout), bronchial lumen diameter (Bin), bronchial wall thickness (Bwt) and adjacent artery diameter (A); and computes Bout/A, Bin/A and Bwt/A for each BA pair from the segmental bronchi to the last visible generation. Three datasets were used to validate the automatic BA analysis. First BA analysis was executed on 23 manually annotated CT scans (11 CF, 12 control subjects) to compare automatic with manual BA-analysis outcomes. Furthermore, the BA analysis was executed on two longitudinal datasets (Copenhagen 111 CTs, ataluren 347 CTs) to assess longitudinal BA changes and compare them with manual scoring results.
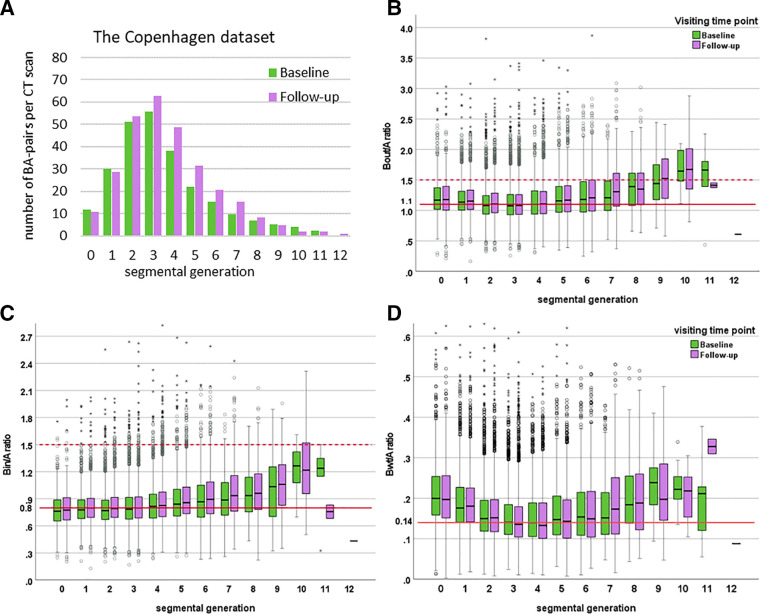
Results: The automatic and manual BA analysis showed no significant differences in quantifying bronchi. For the longitudinal datasets the automatic BA analysis detected 247 and 347 BA pairs/CT in the Copenhagen and ataluren dataset, respectively. A significant increase of 0.02 of Bout/A and Bin/A was detected for Copenhagen dataset over an interval of 2 years, and 0.03 of Bout/A and 0.02 of Bin/A for ataluren dataset over an interval of 48 weeks (all p<0.001). The progression of 0.01 of Bwt/A was detected only in the ataluren dataset (p<0.001). BA-analysis outcomes showed weak to strong correlations (correlation coefficient from 0.29 to 0.84) with manual scoring results for airway disease.
Conclusion: The BA analysis can fully automatically analyse a large number of BA pairs on chest CTs to detect and monitor progression of bronchial wall thickening and bronchial widening in patients with CF.
Keywords: Bronchiectasis; Cystic Fibrosis; Imaging/CT MRI etc; Paediatric Lung Disaese.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: HT has received in the last 5 years multiple grants from the following public and institutional grant institutions for lung structure and function research: NHMRC, NIH, CFF, ECFS, IMI, Sophia Foundation. He received unconditional grants for investigator-initiated research from Chiesi; Vectura, Novartis and Insmed. He has acted as consultant for Insmed, TBIO, Thirona, Neupharma and Boehringer. He has a part time position as chief medical officer for Thirona. He functions as vice chair and faculty for the Advance course sponsored by Vertex. He owns no shares. LG-E is a scientist working at Thirona. JPC is shareholder at Thirona. DC is director of the Erasmus MC-LungAnalysis laboratory. PC acted as consultant for Vertex and Chiesi Pharmaceuticals.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials