

Higher pelvic incidence values are a risk factor for trans-iliac trans-sacral screw malposition in sacroiliac complex fracture treatment
- PMID: 37735320
- PMCID: PMC10513998
- DOI: 10.1186/s10195-023-00728-0
Higher pelvic incidence values are a risk factor for trans-iliac trans-sacral screw malposition in sacroiliac complex fracture treatment
Abstract
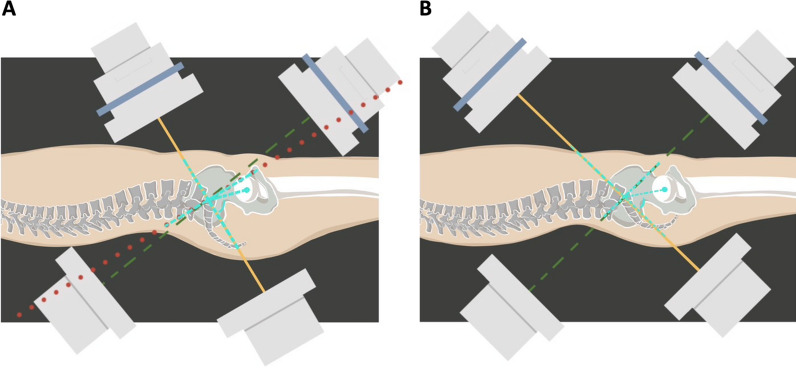
Background: Percutaneous iliosacral (IS) screw fixation and trans-iliac trans-sacral (TITS) screw fixation are clinically effective treatments of posterior pelvic sacroiliac fractures. In order to accurately assess the sacrum position relative to the pelvis, pelvic incidence (PI) is a commonly utilized radiographic parameter in sagittal view. This study aimed to investigate and compare the surgical outcomes and radiographic parameters of IS or TITS screw fixations for the treatment of posterior sacroiliac complex fractures with different PI values.
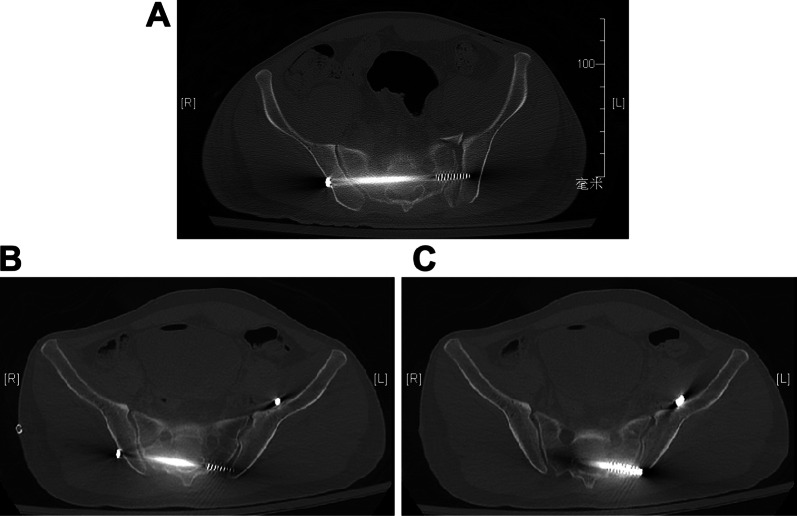
Materials and methods: The data on patients with posterior pelvic sacroiliac fractures who underwent percutaneous IS or TITS screw fixations, or both, at a single level I trauma center between January 2017 and June 2020 were reviewed. We documented the patient characteristics and fracture types, reviewed surgical records, and measured the radiographic parameters via plain films and multi-planar computed tomography (mpCT) images. Radiographic variations in PI, sacral slope, pelvic tilt, sacral dysmorphism, pelvic ring reduction quality, screw deviation angles, screw malposition grading, and iatrogenic complications were documented and analyzed.
Results: A total of 85 patients were included, and 65 IS and 70 TITS screws were accounted for. Patients were divided into two groups according to screw fixation method and further divided into four sub-groups based on baseline PI values. The PI cutoff values were 49.85° and 48.05° in the IS and TITS screw groups, respectively, according to receiver operating characteristic analysis and Youden's J statistic. Smaller PI values were significantly correlated with sacral dysmorphism (p = 0.027 and 0.003 in the IS and TITS screw groups, respectively). Patients with larger PI values were at a significantly increased risk of screw malposition in the TITS screw group (p = 0.049), with no association in the IS screw group. Logistic regression confirmed that a larger PI value was a significant risk factor for screw malposition in the TITS screw group (p = 0.010). The post-operative outcomes improved from poor/fair (at 6 months) to good/average (at 12 months) based on the Postel Merle d'Aubigné and Majeed scores, with no significant differences between subgroups.
Conclusions: Both percutaneous IS and TITS screw fixations are safe and effective treatments for posterior pelvic sacroiliac fractures. Due to the higher risk of screw malposition in patients with larger PI values, it is crucial to identify potential patients at risk when performing TITS screw fixation surgery.
Level of evidence: Level III.
Keywords: Iliosacral screw; Pelvic fracture; Pelvic incidence; Trans-iliac trans-sacral screw.
© 2023. Societa Italiana di Ortopedia e Traumatologia (Italian Society of Orthopaedics and Traumatology SIOT).
Conflict of interest statement
The authors declare no conflicts of interest for this work.
Figures
References
-
- Cullinane DC, Schiller HJ, Zielinski MD et al (2011) Eastern Association for the Surgery of Trauma Practice Management guidelines for hemorrhage in pelvic fracture—update and systematic review. J Trauma 71:1850–1868. 10.1097/TA.0b013e31823dca9a - PubMed
-
- Arvieux C, Thony F, Broux C et al (2012) Current management of severe pelvic and perineal trauma. J Visc Surg 149:e227–238. 10.1016/j.jviscsurg.2012.06.004 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
