

How an emergency department is organized to provide opioid-specific harm reduction and facilitators and barriers to harm reduction implementation: a systems perspective
- PMID: 37735432
- PMCID: PMC10515241
- DOI: 10.1186/s12954-023-00871-1
How an emergency department is organized to provide opioid-specific harm reduction and facilitators and barriers to harm reduction implementation: a systems perspective
Abstract
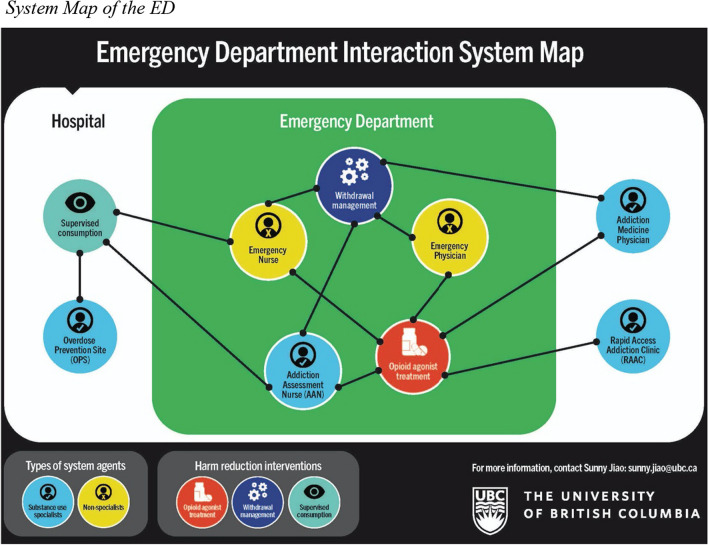
Background: The intersection of dual public health emergencies-the COVID-19 pandemic and the drug toxicity crisis-has led to an urgent need for acute care based harm reduction for unregulated opioid use. Emergency Departments (EDs) as Complex Adaptive Systems (CASs) with multiple, interdependent, and interacting elements are suited to deliver such interventions. This paper examines how the ED is organized to provide harm reduction and identifies facilitators and barriers to implementation in light of interactions between system elements.
Methods: Using a case study design, we conducted interviews with Emergency Physicians (n = 5), Emergency Nurses (n = 10), and clinical leaders (n = 5). Nine organizational policy documents were also collected. Interview data were analysed using a Reflexive Thematic Analysis approach. Policy documents were analysed using a predetermined coding structure pertaining to staffing roles and responsibilities and the interrelationships therein for the delivery of opioid-specific harm reduction in the ED. The theory of CAS informed data analysis.
Results: An array of system agents, including substance use specialist providers and non-specialist providers, interacted in ways that enable the provision of harm reduction interventions in the ED, including opioid agonist treatment, supervised consumption, and withdrawal management. However, limited access to specialist providers, when coupled with specialist control, non-specialist reliance, and concerns related to safety, created tensions in the system that hinder harm reduction provision with resulting implications for the delivery of care.
Conclusions: To advance harm reduction implementation, there is a need for substance use specialist services that are congruent with the 24 h a day service delivery model of the ED, and for organizational policies that are attentive to discourses of specialized practice, hierarchical relations of power, and the dynamic regulatory landscape. Implementation efforts that take into consideration these perspectives have the potential to reduce harms experienced by people who use unregulated opioids, not only through overdose prevention and improving access to safer opioid alternatives, but also through supporting people to complete their unique care journeys.
Keywords: Acute care; Complex adaptive systems; Emergency department; Harm reduction; Opioid agonist treatment; Supervised consumption; Unregulated substance use; Withdrawal management.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Ministry of Public Safety & Solicitor General. Illicit drug toxicity deaths in BC: January 1, 2012–June 30, 2022. 2022. https://www2.gov.bc.ca/assets/gov/birth-adoption-death-marriage-and-divo.... Accessed 30 Aug 2022.
-
- Province of British Columbia. Provincial health officer declares public health emergency. 2016. https://news.gov.bc.ca/releases/2016HLTH0026-000568
-
- Province of British Columbia. Province declares state of emergency to support COVID-19 responses. 2020 [cited 2022 September 27]. https://news.gov.bc.ca/releases/2020PSSG0017-000511
-
- Canadian Centre on Substance Use and Addiction. Impacts of the COVID-19 pandemic on people who use substances: what we heard. 2020. https://www.ccsa.ca/sites/default/files/2020-07/CCSA-COVID-19-Impacts-on.... Accessed 27 Sept 2022.
-
- Legislatively Assembly of British Columbia. Closing gaps, reducing barriers: Expanding the response to the toxic drug and overdose crisis. Select Standing Committee on Health. 2022. https://www.leg.bc.ca/content/CommitteeDocuments/42nd-parliament/3rd-ses.... Accessed 15 Dec 2022.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
