

Implementation of coordinated spontaneous awakening and breathing trials using telehealth-enabled, real-time audit and feedback for clinician adherence (TEACH): a type II hybrid effectiveness-implementation cluster-randomized trial
- PMID: 37735443
- PMCID: PMC10515061
- DOI: 10.1186/s13012-023-01303-1
Implementation of coordinated spontaneous awakening and breathing trials using telehealth-enabled, real-time audit and feedback for clinician adherence (TEACH): a type II hybrid effectiveness-implementation cluster-randomized trial
Abstract
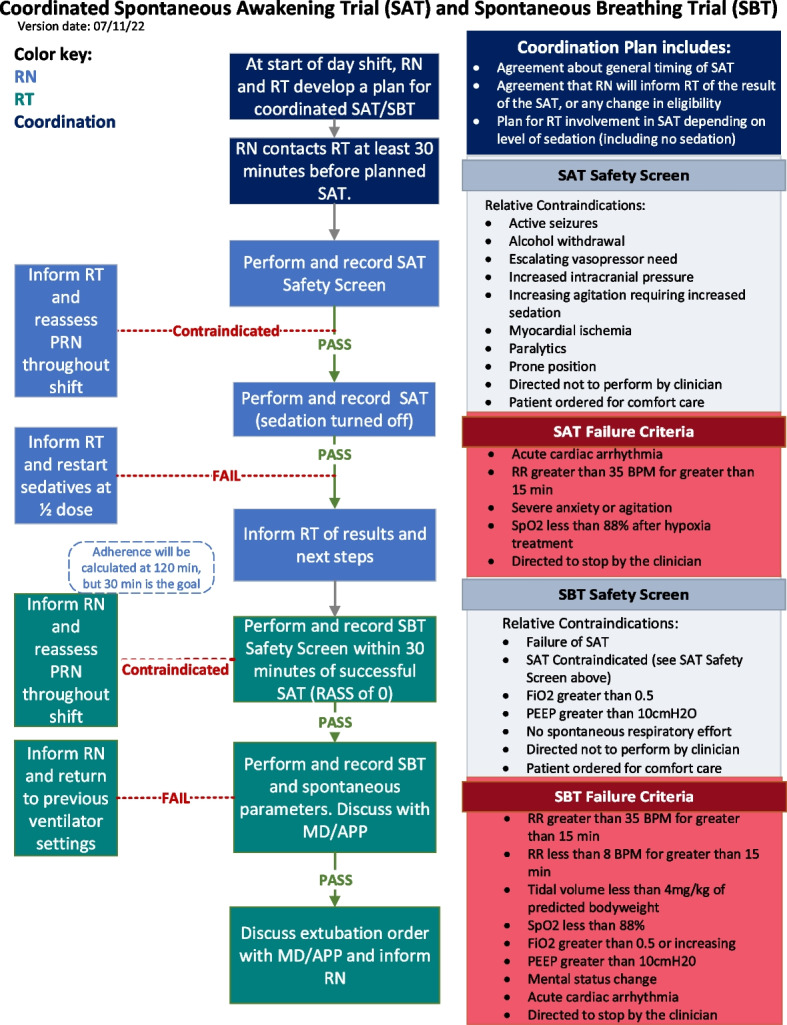
Background: Intensive care unit (ICU) patients on mechanical ventilation often require sedation and analgesia to improve comfort and decrease pain. Prolonged sedation and analgesia, however, may increase time on mechanical ventilation, risk for ventilator associated pneumonia, and delirium. Coordinated interruptions in sedation [spontaneous awakening trials (SATs)] and spontaneous breathing trials (SBTs) increase ventilator-free days and improve mortality. Coordination of SATs and SBTs is difficult with substantial implementation barriers due to difficult-to-execute sequencing between nurses and respiratory therapists. Telehealth-enabled remote care has the potential to overcome these barriers and improve coordinated SAT and SBT adherence by enabling proactive high-risk patient monitoring, surveillance, and real-time assistance to frontline ICU teams.
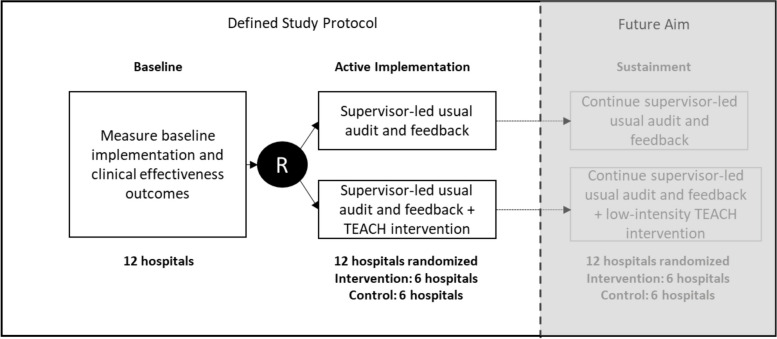
Methods: The telehealth-enabled, real-time audit and feedback for clinician adherence (TEACH) study will determine whether adding a telehealth augmented real-time audit and feedback to a usual supervisor-led audit and feedback intervention will yield higher coordinated SAT and SBT adherence and more ventilator-free days in mechanically ventilated patients than a usual supervisor-led audit and feedback intervention alone in a type II hybrid effectiveness-implementation cluster-randomized clinical trial in 12 Intermountain Health hospitals with 15 ICUs. In the active comparator control group (six hospitals), the only intervention is the usual supervisor-led audit and feedback implementation. The telehealth-enabled support (TEACH) intervention in six hospitals adds real-time identification of patients eligible for a coordinated SAT and SBT and consultative input from telehealth respiratory therapists, nurses, and physicians to the bedside clinicians to promote adherence including real-time assistance with execution. All intubated and mechanically ventilated patients ≥ 16 years of age are eligible for enrollment except for patients who die on the day of intubation or have preexisting brain death. Based on preliminary power analyses, we plan a 36-month intervention period that includes a 90-day run-in period. Estimated enrollment in the final analysis is up to 9900 mechanically ventilated patients over 33 months.
Discussion: The TEACH study will enhance implementation science by providing insight into how a telehealth intervention augmenting a usual audit and feedback implementation may improve adherence to coordinated SAT and SBT and increase ventilator-free days.
Trial registration: Clinicaltrials.gov, NCT05141396 , registered 12/02/2021.
Keywords: Audit and feedback; Hybrid effectiveness-implementation trials; Implementation; Mechanical ventilation; Spontaneous awakening trials; Spontaneous breathing trials; Telehealth.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
IDP reports grants from the National Institutes of Health, Centers for Disease Control and Prevention, and Janssen Pharmaceuticals and funding to his institution from Regeneron and Asahi Kasei Pharma. RS reports grants from the National Institutes of Health, the Agency for Healthcare Research, the Centers for Disease Control and Prevention, and the Patient-Centered Research Outcomes Institute. RS is also a physician founder of the IPASS Patient Safety Institute, and his equity is owned by his employer, Intermountain Health. RH reports grants from the National Institutes of Health and consulting (DSMB member) for Pfizer. CKG report grants from the National Institutes of Health. Other authors declare that they have no competing interests.
Figures
Similar articles
-
Awakening and Breathing Coordination: A Mixed-Methods Analysis of Determinants of Implementation.Ann Am Thorac Soc. 2023 Oct;20(10):1483-1490. doi: 10.1513/AnnalsATS.202212-1048OC. Ann Am Thorac Soc. 2023. PMID: 37413692 Free PMC article.
-
Comparison of SAT and SBT Conduct During the ABC Trial and PILOT Trial.J Intensive Care Med. 2025 Jan;40(1):3-9. doi: 10.1177/08850666231213337. Epub 2023 Nov 19. J Intensive Care Med. 2025. PMID: 37981753 Free PMC article. Clinical Trial.
-
Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial.Lancet. 2008 Jan 12;371(9607):126-34. doi: 10.1016/S0140-6736(08)60105-1. Lancet. 2008. PMID: 18191684 Clinical Trial.
-
Pairing Spontaneous Awakening and Breathing Trials to Improve Weaning of Intensive Care Unit Patients: A Systematic Review.Crit Care Nurs Q. 2025 Jul-Sep 01;48(3):237-256. doi: 10.1097/CNQ.0000000000000551. Epub 2025 May 21. Crit Care Nurs Q. 2025. PMID: 40423382
-
ABCDE and ABCDEF care bundles: A systematic review of the implementation process in intensive care units.Medicine (Baltimore). 2022 Jun 24;101(25):e29499. doi: 10.1097/MD.0000000000029499. Medicine (Baltimore). 2022. PMID: 35758388 Free PMC article.
Cited by
-
Research Accomplishments in Pulmonary, Critical Care, and Sleep: A Retrospective Review.Am J Respir Crit Care Med. 2023 Dec 15;208(12):1268-1270. doi: 10.1164/rccm.202311-2047PP. Am J Respir Crit Care Med. 2023. PMID: 37966304 Free PMC article. No abstract available.
-
Normalizing daily awakening and breathing coordination at 15 heterogenous ICUs: a multicenter post-implementation survey.Implement Sci Commun. 2025 Aug 25;6(1):91. doi: 10.1186/s43058-025-00770-5. Implement Sci Commun. 2025. PMID: 40855450 Free PMC article.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
