

Novel therapeutics and future directions for refractory immune thrombocytopenia
- PMID: 37735554
- PMCID: PMC11101754
- DOI: 10.1111/bjh.19078
Novel therapeutics and future directions for refractory immune thrombocytopenia
Abstract
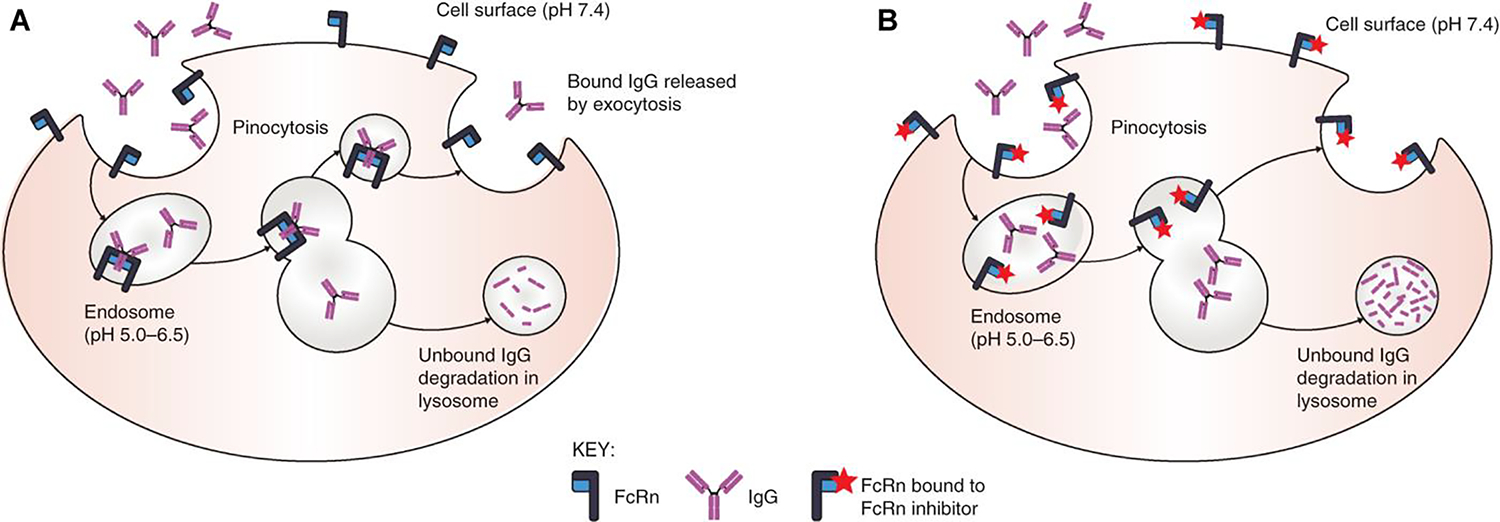
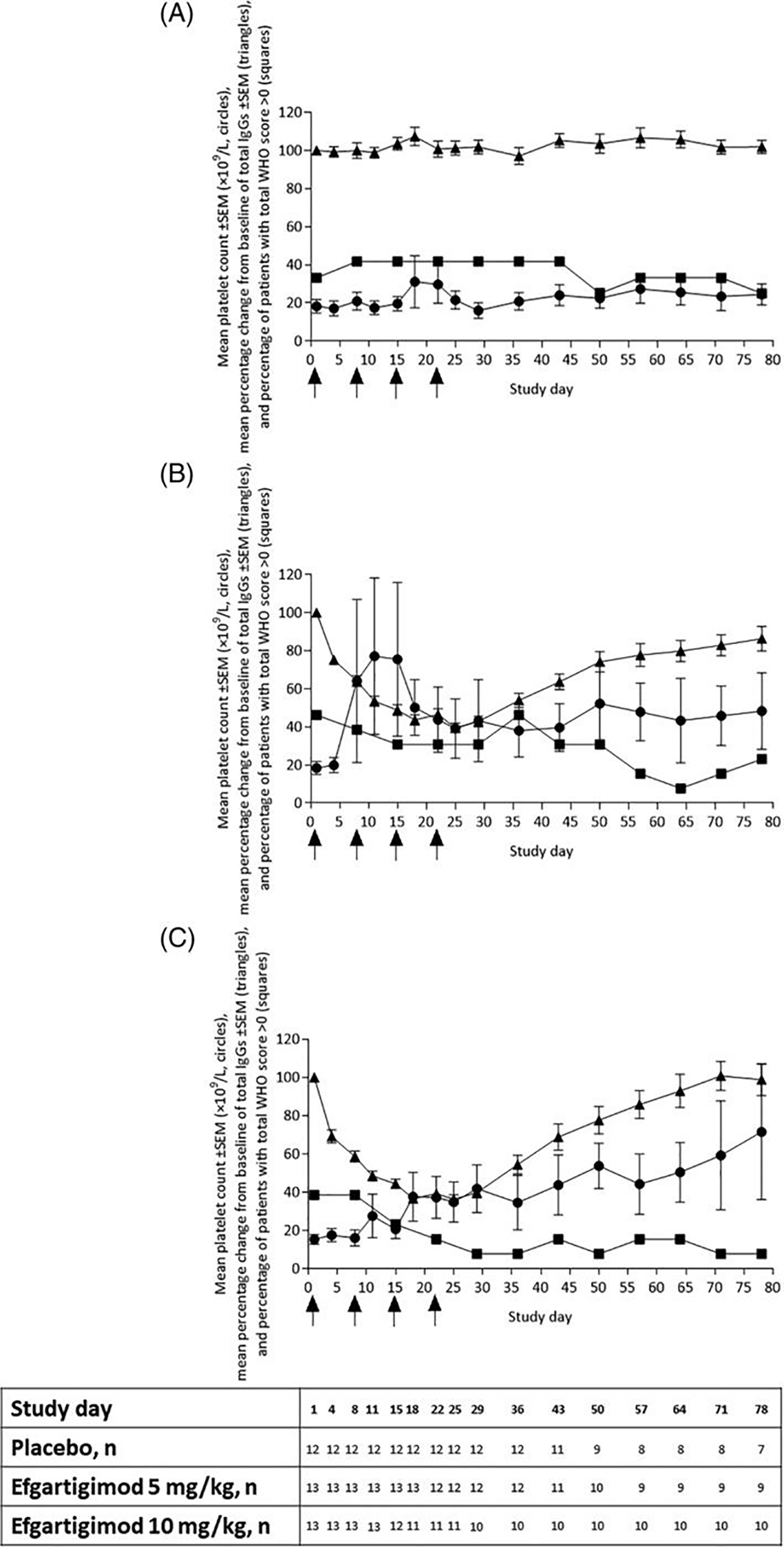
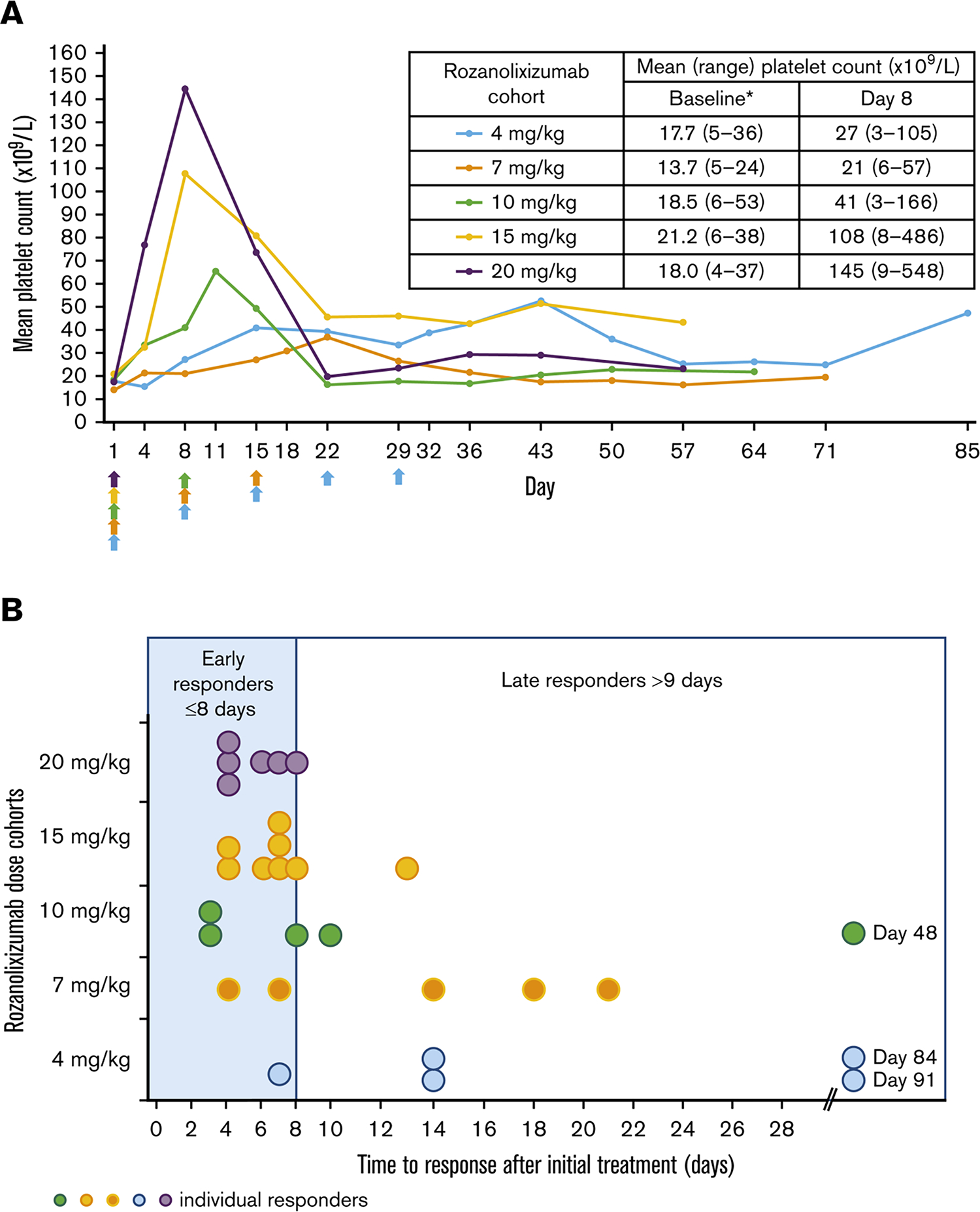
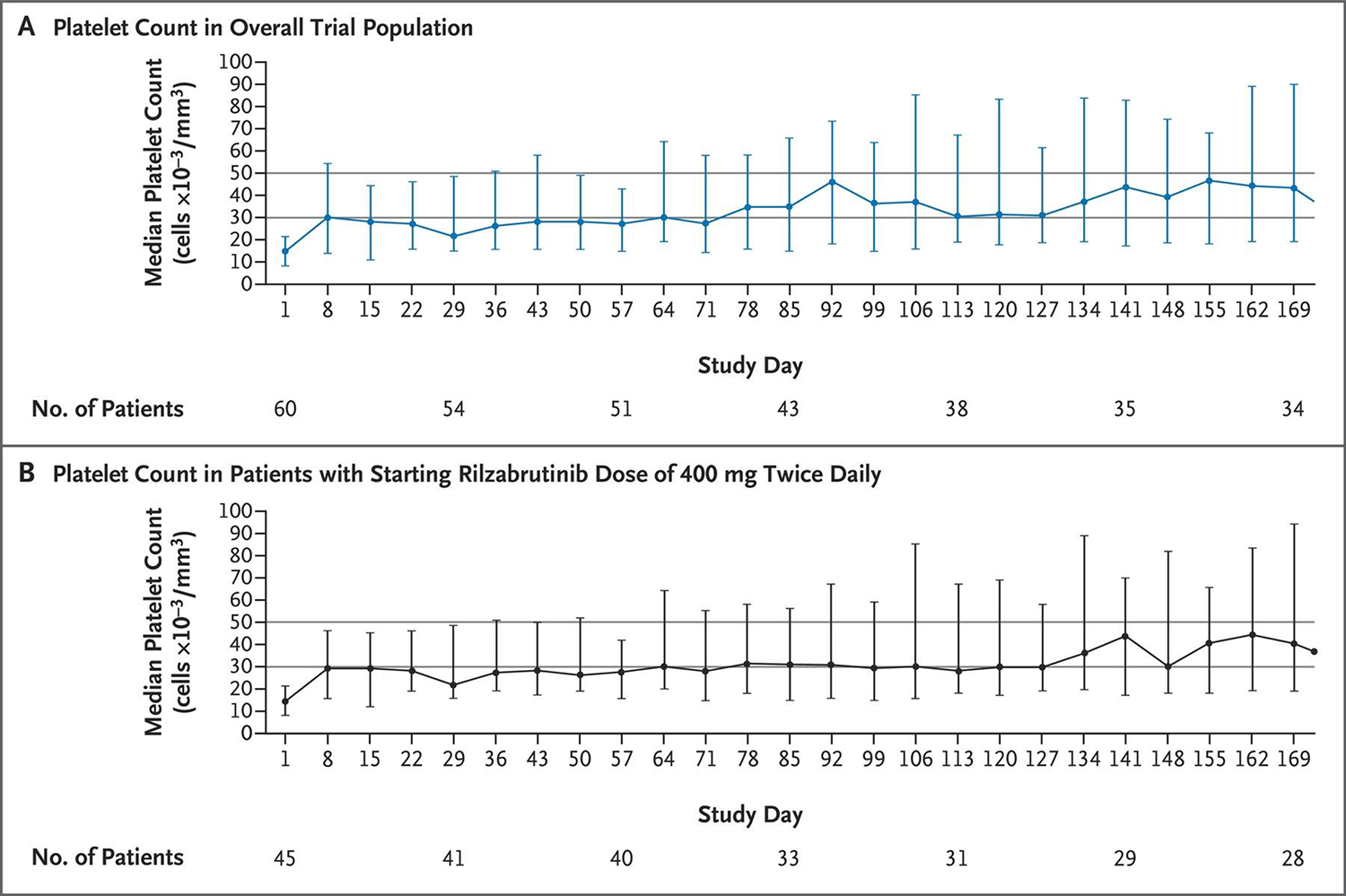
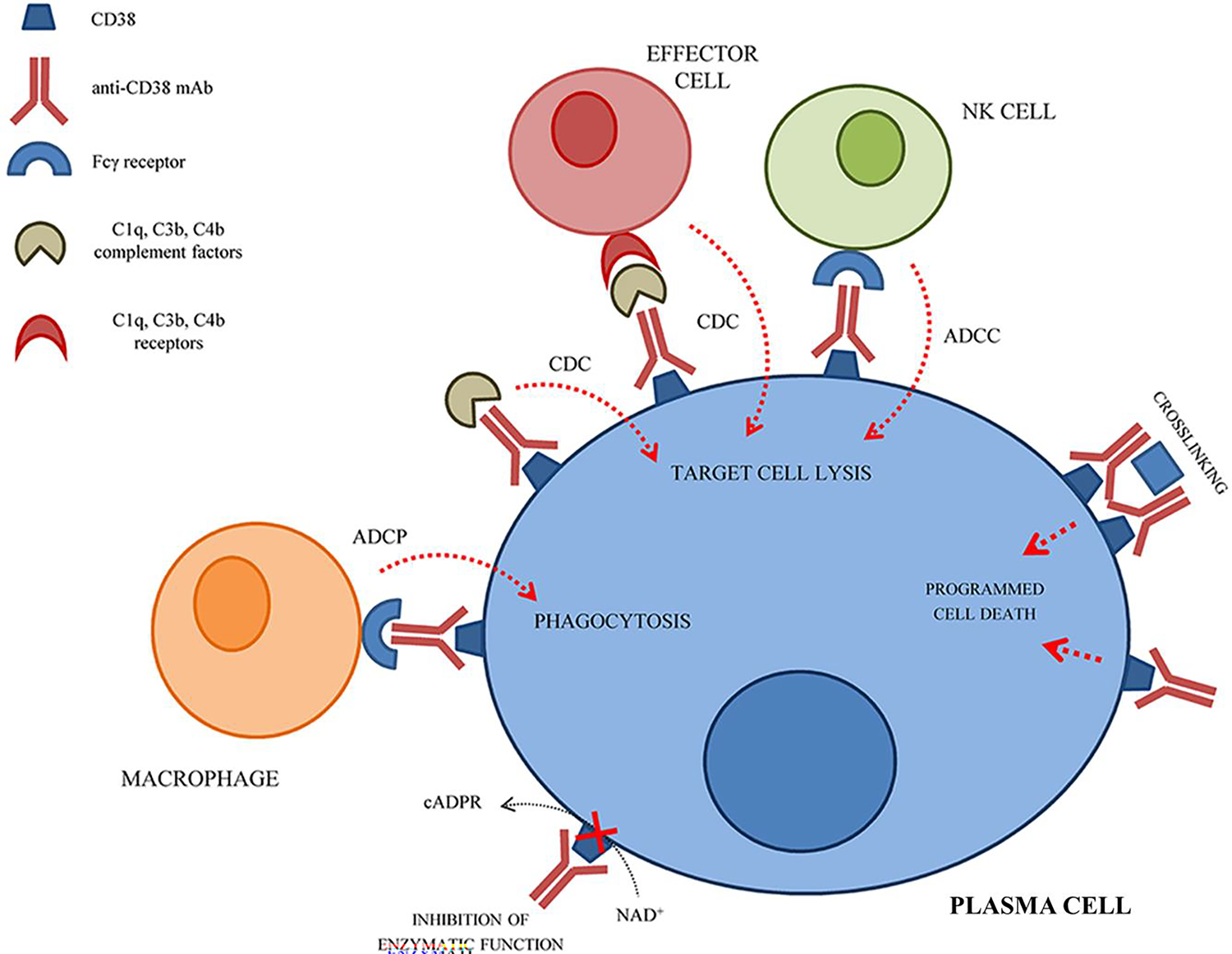
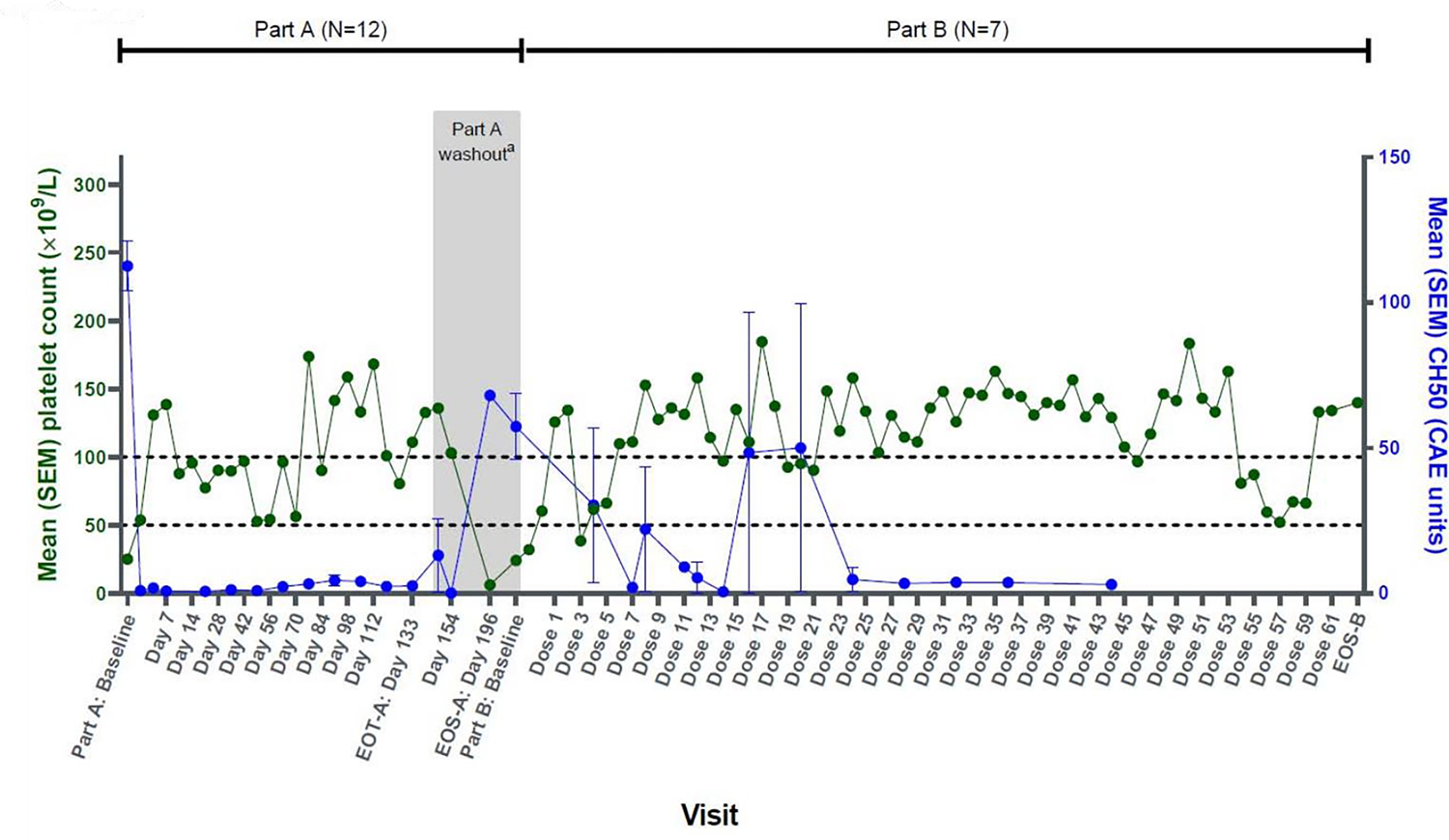
Immune thrombocytopenia (ITP) is an autoimmune bleeding disorder affecting approximately 1 in 20 000 people. While most patients with ITP are successfully managed with the current set of standard and approved therapeutics, patients who cannot be adequately managed with these therapies, considered to have refractory ITP, are not uncommon. Therefore, there remains an ongoing need for novel therapeutics and drug development in ITP. Several agents exploiting novel targets and mechanisms in ITP are presently under clinical development, with trials primarily recruiting heavily pretreated patients and those with otherwise refractory disease. Such agents include the neonatal Fc receptor antagonist efgartigimod, the Bruton tyrosine kinase inhibitor rilzabrutinib, the complement inhibitors sutimlimab and iptacopan and anti-CD38 monoclonal antibodies such as daratumumab and mezagitamab, among others. Each of these agents exploits therapeutic targets or other aspects of ITP pathophysiology currently not targeted by the existing approved agents (thrombopoietin receptor agonists and fostamatinib). This manuscript offers an in-depth review of the current available data for novel therapeutics in ITP presently undergoing phase 2 or 3 studies in patients with heavily pretreated or refractory ITP. It additionally highlights the future directions for drug development in refractory ITP, including discussion of innovative clinical trial designs, health-related quality of life as an indispensable clinical trial end-point and balancing potential toxicities of drugs with their potential benefits in a bleeding disorder in which few patients suffer life-threatening bleeding.
Keywords: daratumumab; efgartigimod; immune thrombocytopenia; iptacopan; mezagitamab; platelets; refractory; rilzabrutinib; rozanolixizumab; sutimlimab; umbrella trials.
© 2023 British Society for Haematology and John Wiley & Sons Ltd.
Conflict of interest statement
Figures
References
-
- Al-Samkari H, Kuter DJ. Immune Thrombocytopenia in Adults: Modern Approaches to Diagnosis and Treatment. Semin Thromb Hemost. 2020;46(3):275–88. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
