

Consequences of group III/IV afferent feedback and respiratory muscle work on exercise tolerance in heart failure with reduced ejection fraction
- PMID: 37735814
- PMCID: PMC10900130
- DOI: 10.1113/EP090755
Consequences of group III/IV afferent feedback and respiratory muscle work on exercise tolerance in heart failure with reduced ejection fraction
Abstract
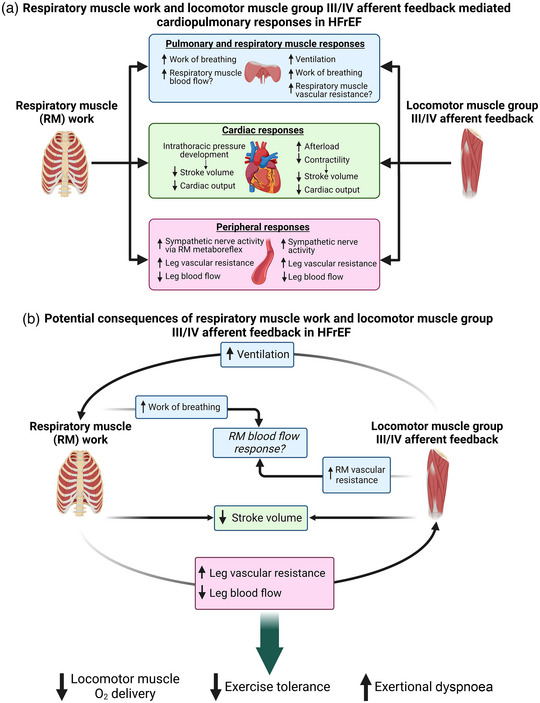
Exercise intolerance and exertional dyspnoea are the cardinal symptoms of heart failure with reduced ejection fraction (HFrEF). In HFrEF, abnormal autonomic and cardiopulmonary responses arising from locomotor muscle group III/IV afferent feedback is one of the primary mechanisms contributing to exercise intolerance. HFrEF patients also have pulmonary system and respiratory muscle abnormalities that impair exercise tolerance. Thus, the primary impetus for this review was to describe the mechanistic consequences of locomotor muscle group III/IV afferent feedback and respiratory muscle work in HFrEF. To address this, we first discuss the abnormal autonomic and cardiopulmonary responses mediated by locomotor muscle afferent feedback in HFrEF. Next, we outline how respiratory muscle work impairs exercise tolerance in HFrEF through its effects on locomotor muscle O2 delivery. We then discuss the direct and indirect evidence supporting an interaction between locomotor muscle group III/IV afferent feedback and respiratory muscle work during exercise in HFrEF. Last, we outline future research directions related to locomotor and respiratory muscle abnormalities to progress the field forward in understanding the pathophysiology of exercise intolerance in HFrEF. NEW FINDINGS: What is the topic of this review? This review is focused on understanding the role that locomotor muscle group III/IV afferent feedback and respiratory muscle work play in the pathophysiology of exercise intolerance in patients with heart failure. What advances does it highlight? This review proposes that the concomitant effects of locomotor muscle afferent feedback and respiratory muscle work worsen exercise tolerance and exacerbate exertional dyspnoea in patients with heart failure.
Keywords: diaphragm; exercise pressor reflex; metaboreflex; respiratory muscle blood flow.
© 2023 The Authors. Experimental Physiology published by John Wiley & Sons Ltd on behalf of The Physiological Society.
Conflict of interest statement
The authors have no conflicts of interest to report for this manuscript.
Figures
Similar articles
-
Locomotor muscle group III/IV afferents constrain stroke volume and contribute to exercise intolerance in human heart failure.J Physiol. 2020 Dec;598(23):5379-5390. doi: 10.1113/JP280333. Epub 2020 Sep 23. J Physiol. 2020. PMID: 32886795 Free PMC article.
-
Influence of locomotor muscle group III/IV afferents on cardiovascular and ventilatory responses in human heart failure during submaximal exercise.J Appl Physiol (1985). 2022 Apr 1;132(4):903-914. doi: 10.1152/japplphysiol.00371.2021. Epub 2022 Feb 24. J Appl Physiol (1985). 2022. PMID: 35201931 Free PMC article.
-
Metabo- and mechanoreceptor expression in human heart failure: Relationships with the locomotor muscle afferent influence on exercise responses.Exp Physiol. 2020 May;105(5):809-818. doi: 10.1113/EP088353. Epub 2020 Mar 29. Exp Physiol. 2020. PMID: 32105387 Free PMC article.
-
Impaired Exercise Tolerance in Heart Failure: Role of Skeletal Muscle Morphology and Function.Curr Heart Fail Rep. 2018 Dec;15(6):323-331. doi: 10.1007/s11897-018-0408-6. Curr Heart Fail Rep. 2018. PMID: 30178183 Free PMC article. Review.
-
Muscle sympathetic activity in resting and exercising humans with and without heart failure.Appl Physiol Nutr Metab. 2015 Nov;40(11):1107-15. doi: 10.1139/apnm-2015-0289. Epub 2015 Aug 14. Appl Physiol Nutr Metab. 2015. PMID: 26481289 Review.
Cited by
-
Tidal Volume Challenge to Assess Volume Responsiveness with Dynamic Preload Indices During Non-Cardiac Surgery: A Prospective Study.J Clin Med. 2024 Dec 27;14(1):101. doi: 10.3390/jcm14010101. J Clin Med. 2024. PMID: 39797182 Free PMC article.
-
Exaggerated Inspiratory Muscle Metaboreflex in Arterial Hypertension.J Am Heart Assoc. 2024 Jun 4;13(11):e033511. doi: 10.1161/JAHA.123.033511. Epub 2024 May 28. J Am Heart Assoc. 2024. PMID: 38804227 Free PMC article. No abstract available.
References
-
- Aaron, E. A. , Seow, K. C. , Johnson, B. D. , & Dempsey, J. A. (1992). Oxygen cost of exercise hyperpnea: Implications for performance. Journal of Applied Physiology, 72(5), 1818–1825. - PubMed
-
- Aimo, A. , Saccaro, L. F. , Borrelli, C. , Fabiani, I. , Gentile, F. , Passino, C. , Emdin, M. , Piepoli, M. F. , Coats, A. J. S. , & Giannoni, A. (2021). The ergoreflex: How the skeletal muscle modulates ventilation and cardiovascular function in health and disease. European Journal of Heart Failure, 23(9), 1458–1467. - PMC - PubMed
-
- Amann, M. , Runnels, S. , Morgan, D. E. , Trinity, J. D. , Fjeldstad, A. S. , Wray, D. W. , Reese, V. R. , & Richardson, R. S. (2011). On the contribution of group III and IV muscle afferents to the circulatory response to rhythmic exercise in humans. The Journal of Physiology, 589(15), 3855–3866. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical