

Commissural alignment in the Evolut TAVR procedure: conventional versus hat marker-guided shaft rotation methods
- PMID: 37736211
- PMCID: PMC10507608
- DOI: 10.4244/AIJ-D-23-00017
Commissural alignment in the Evolut TAVR procedure: conventional versus hat marker-guided shaft rotation methods
Abstract
Background: Coronary cannulation after TAVR is sometimes difficult due to an overlap between native and neo-commissures, especially in Evolut devices with a supra-annular position. The Evolut C-tab corresponds to a neo-commissure, and the hat marker is in a fixed position. Therefore, the orientation of the hat marker can be adjusted to minimise overlaps.
Aims: We investigated whether the HAt marker-guided SHaft rotation method (HASH, stylised as the #rotation method) is effective in facilitating coronary artery access after transcatheter aortic valve replacement (TAVR) with an Evolut system.
Methods: We retrospectively analysed 95 patients who underwent electrocardiogram-gated cardiac computed tomography after TAVR. In the #rotation method, the hat marker of the delivery catheter was adjusted to face the greater curvature of the descending thoracic aorta in the left anterior oblique view. Its orientation was maintained while the system passed through the aortic arch.
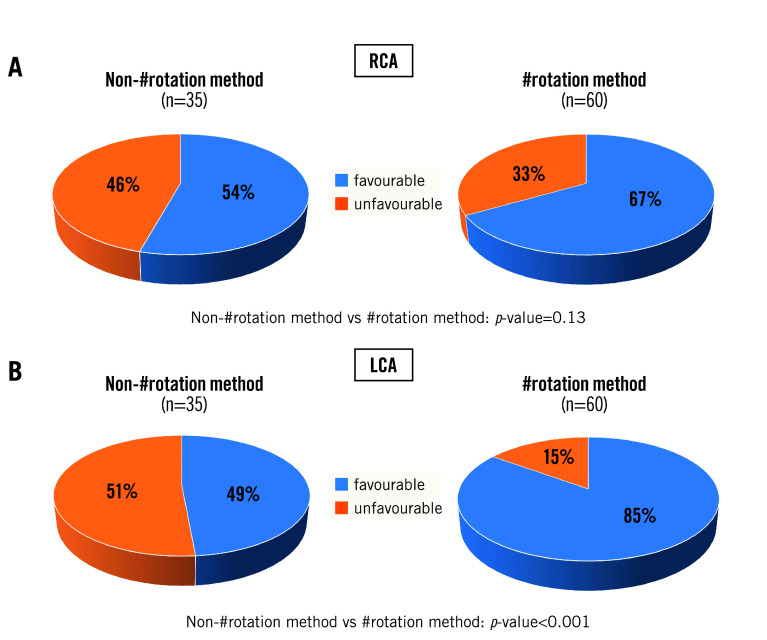
Results: In total, 60 and 35 patients underwent TAVR with the #rotation and non-#rotation methods, respectively. A ±15° angle between the native and neo-commissures was more frequent in the #rotation group (p=0.001). Favourable angles and appropriate frame orientation for access to the left coronary artery were significantly more frequent in the #rotation group than in the non-#rotation group (p<0.001 and p=0.001). Although the #rotation method showed a higher rate of favourable angles and frames in the right coronary artery, statistically significant differences were not found.
Conclusions: The #rotation method is useful for improving commissural post alignment in TAVR with Evolut devices, especially in the ostium of the left coronary artery.
Conflict of interest statement
T. Sakamoto is a clinical proctor of the Evolut TAVR system. The other authors have no conflicts of interest to declare.
Figures





References
-
- Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D, Pocock SJ PARTNER Trial Investigators. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–98. - PubMed
-
- Adams DH, Popma JJ, Reardon MJ, Yakubov SJ, Coselli JS, Deeb GM, Gleason TG, Buchbinder M, Hermiller J, Kleiman NS, Chetcuti S, Heiser J, Merhi W, Zorn G, Tadros P, Robinson N, Petrossian G, Hughes GC, Harrison JK, Conte J, Maini B, Mumtaz M, Chenoweth S, Oh JK U. S. CoreValve Clinical Investigators. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370:1790–8. - PubMed
-
- Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S PARTNER Trial Investigators. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–607. - PubMed
-
- Popma JJ, Adams DH, Reardon MJ, Yakubov SJ, Kleiman NS, Heimansohn D, Hermiller J, Hughes GC, Harrison JK, Coselli J, Diez J, Kafi A, Schreiber T, Gleason TG, Conte J, Buchbinder M, Deeb GM, Carabello B, Serruys PW, Chenoweth S, Oh JK CoreValve United States Clinical Investigators. Transcatheter aortic valve replacement using a self-expanding bioprosthesis in patients with severe aortic stenosis at extreme risk for surgery. J Am Coll Cardiol. 2014;63:1972–81. - PubMed
-
- Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, Thourani VH, Tuzcu EM, Miller DC, Herrmann HC, Doshi D, Cohen DJ, Pichard AD, Kapadia S, Dewey T, Babaliaros V, Szeto WY, Williams MR, Kereiakes D, Zajarias A, Greason KL, Whisenant BK, Hodson RW, Moses JW, Trento A, Brown DL, Fearon WF, Pibarot P, Hahn RT, Jaber WA, Anderson WN, Alu MC, Webb JG PARTNER 2 Investigators. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2016;374:1609–20. - PubMed
LinkOut - more resources
Full Text Sources
Medical