

Hepatic steatosis index at diagnosis has the potential for forecasting end-stage kidney disease in patients with antineutrophil cytoplasmic antibody-associated vasculitis
- PMID: 37736592
- PMCID: PMC10509637
- DOI: 10.4078/jrd.2023.0032
Hepatic steatosis index at diagnosis has the potential for forecasting end-stage kidney disease in patients with antineutrophil cytoplasmic antibody-associated vasculitis
Abstract
Objective: This study evaluated whether the hepatic steatosis index (HSI) at antineutrophil cytoplasmic antibody-associated vasculitis (AAV) diagnosis could forecast poor outcomes during the disease course in AAV patients.
Methods: This study included 260 AAV patients. The equation for HSI is as follows HSI=8×(alanine aminotransferase/aspartate aminotransferase)+body mass index+(2, diabetes mellitus)+(2, female). The cut-off of HSI was obtained using the receiver operating characteristic curve.
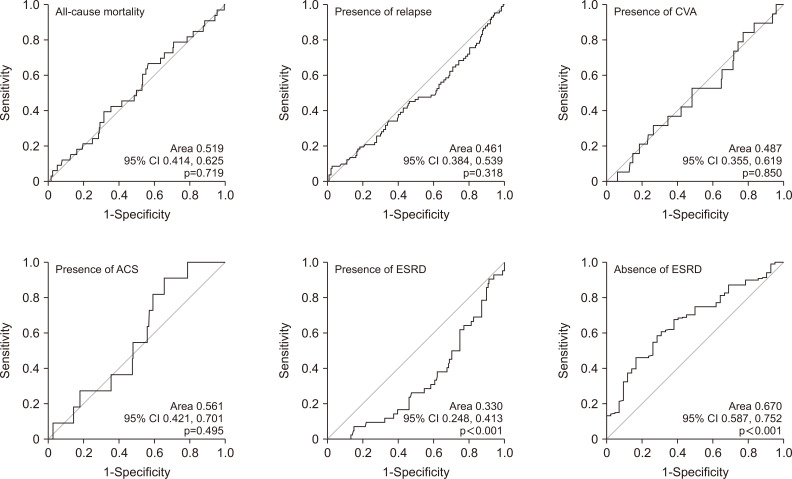
Results: The median age of the 260 patients was 59.5 years, and 65.0% were female. Among the continuous variables excluding the parameters composing the equation for HSI, HSI was significantly correlated with Birmingham vasculitis activity score, five-factor score, haemoglobin, blood urea nitrogen, serum creatinine, and total cholesterol. Among poor outcomes, the area under the curve of HSI for end-stage renal disease (ESRD) was significant, and the cut-off of HSI for ESRD was set at ≤30.82. AAV patients with HSI ≤30.82 exhibited a significantly higher risk of ESRD (relative risk 3.489) and a significantly lower cumulative ESRD-free survival rate than those with HSI >30.82.
Conclusion: This study is the first to demonstrate that HSI at AAV diagnosis could forecast ESRD during the disease course in AAV patients.
Keywords: Antineutrophil cytoplasmic antibody; End-stage renal disease; Forecasting; Hepatic steatosis index; Vasculitis.
Copyright © 2023 by The Korean College of Rheumatology. All rights reserved.
Conflict of interest statement
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
Figures


References
-
- Watts R, Lane S, Hanslik T, Hauser T, Hellmich B, Koldingsnes W, et al. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann Rheum Dis. 2007;66:222–7. doi: 10.1136/ard.2006.054593. - DOI - PMC - PubMed
-
- Guillevin L, Pagnoux C, Seror R, Mahr A, Mouthon L, Toumelin PL French Vasculitis Study Group (FVSG), author The Five-Factor Score revisited: assessment of prognoses of systemic necrotizing vasculitides based on the French Vasculitis Study Group (FVSG) cohort. Medicine (Baltimore) 2011;90:19–27. doi: 10.1097/MD.0b013e318205a4c6. - DOI - PubMed
LinkOut - more resources
Full Text Sources