

The safe zone of distal fibula was determined based on the classification of lateral malleolus fossa
- PMID: 37736730
- PMCID: PMC10514986
- DOI: 10.1186/s13018-023-04194-6
The safe zone of distal fibula was determined based on the classification of lateral malleolus fossa
Abstract
Background: Lateral malleolus fractures are very common, and the distal fibular geometry is complex. This study aimed to classify the lateral malleolus fossa (MF) into different types by characterizing the lateral MF imaging morphology and exploring the relationship between the lateral MF and internal fixation position after distal fibula fractures.
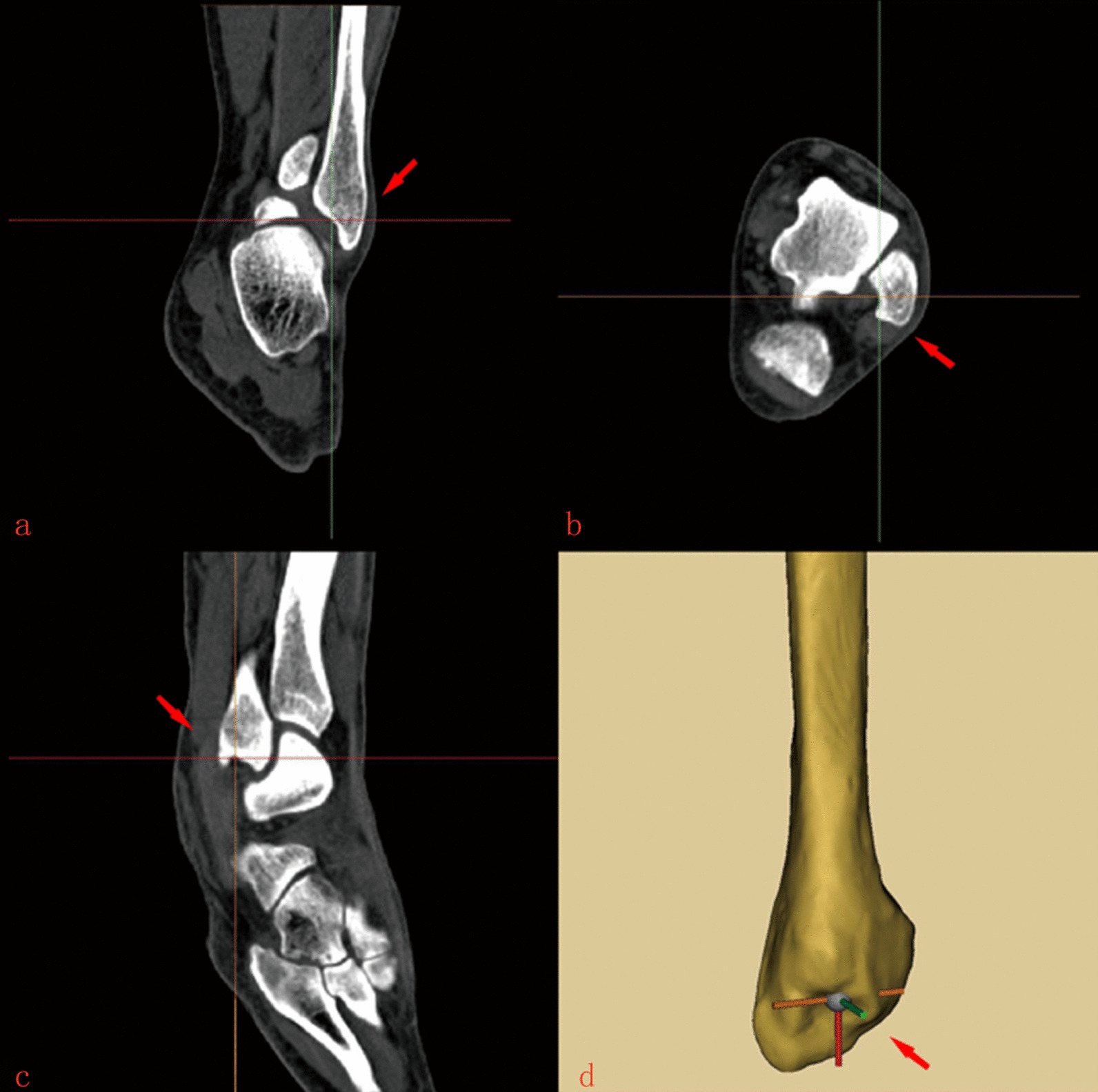
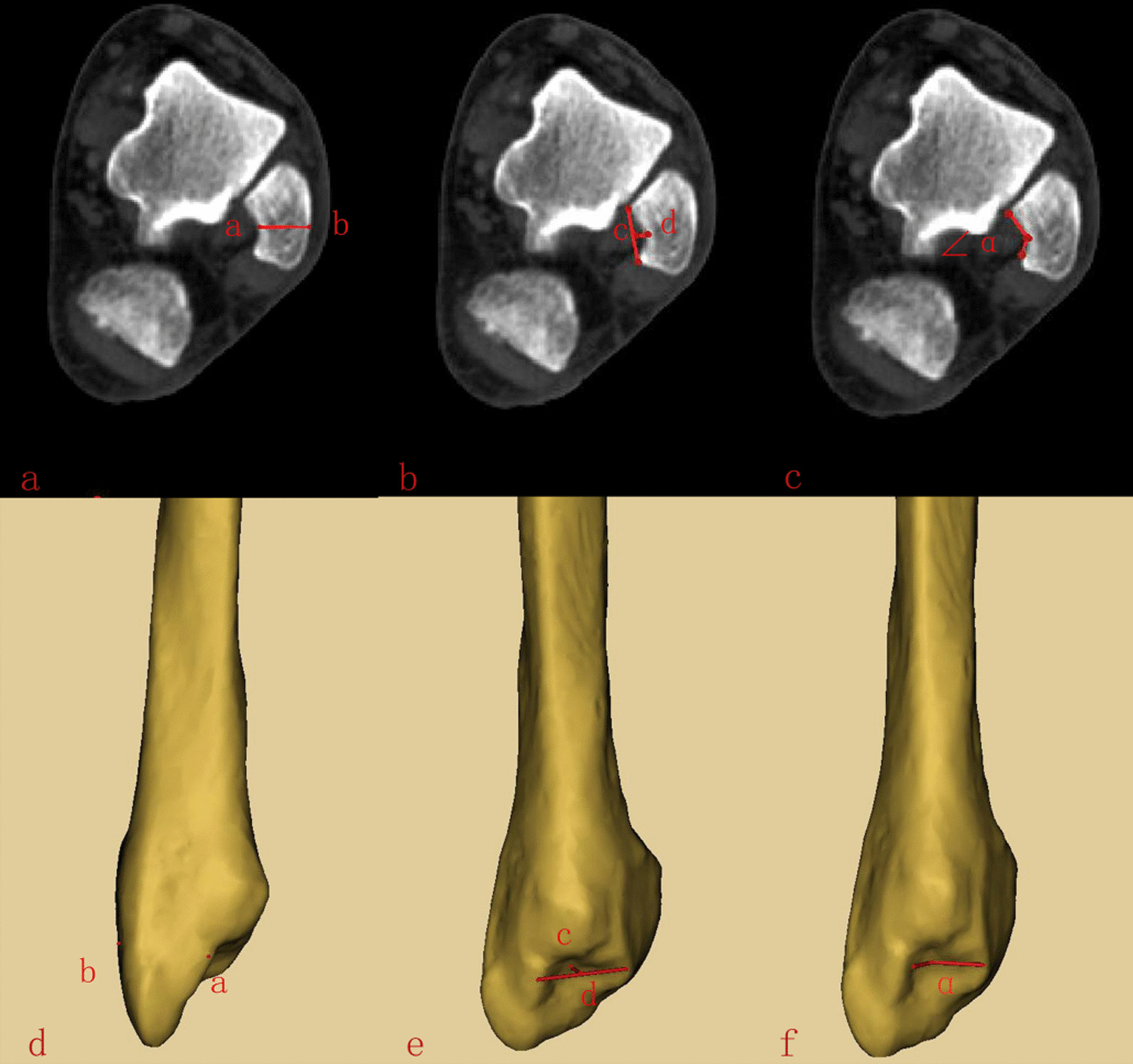
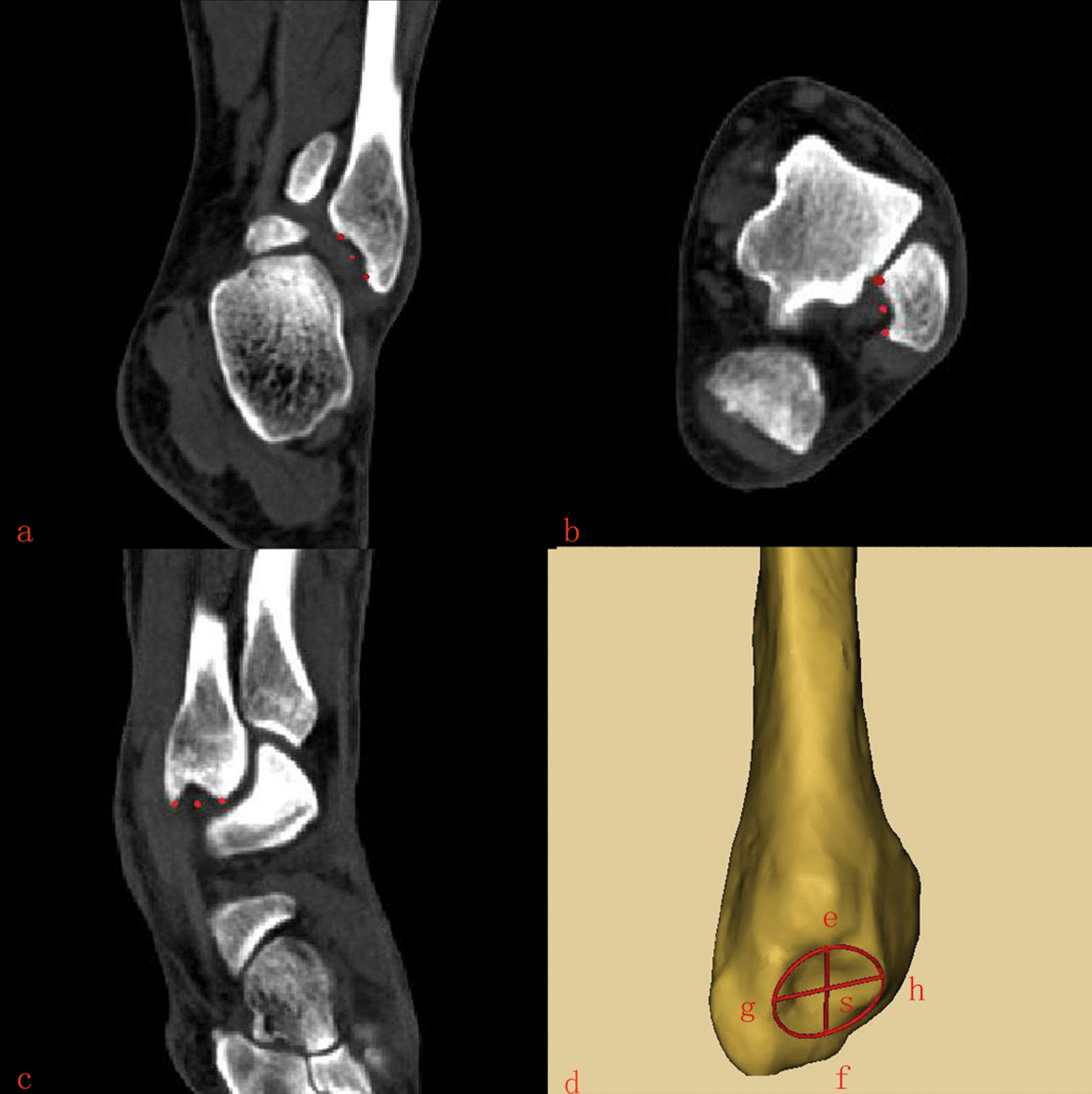
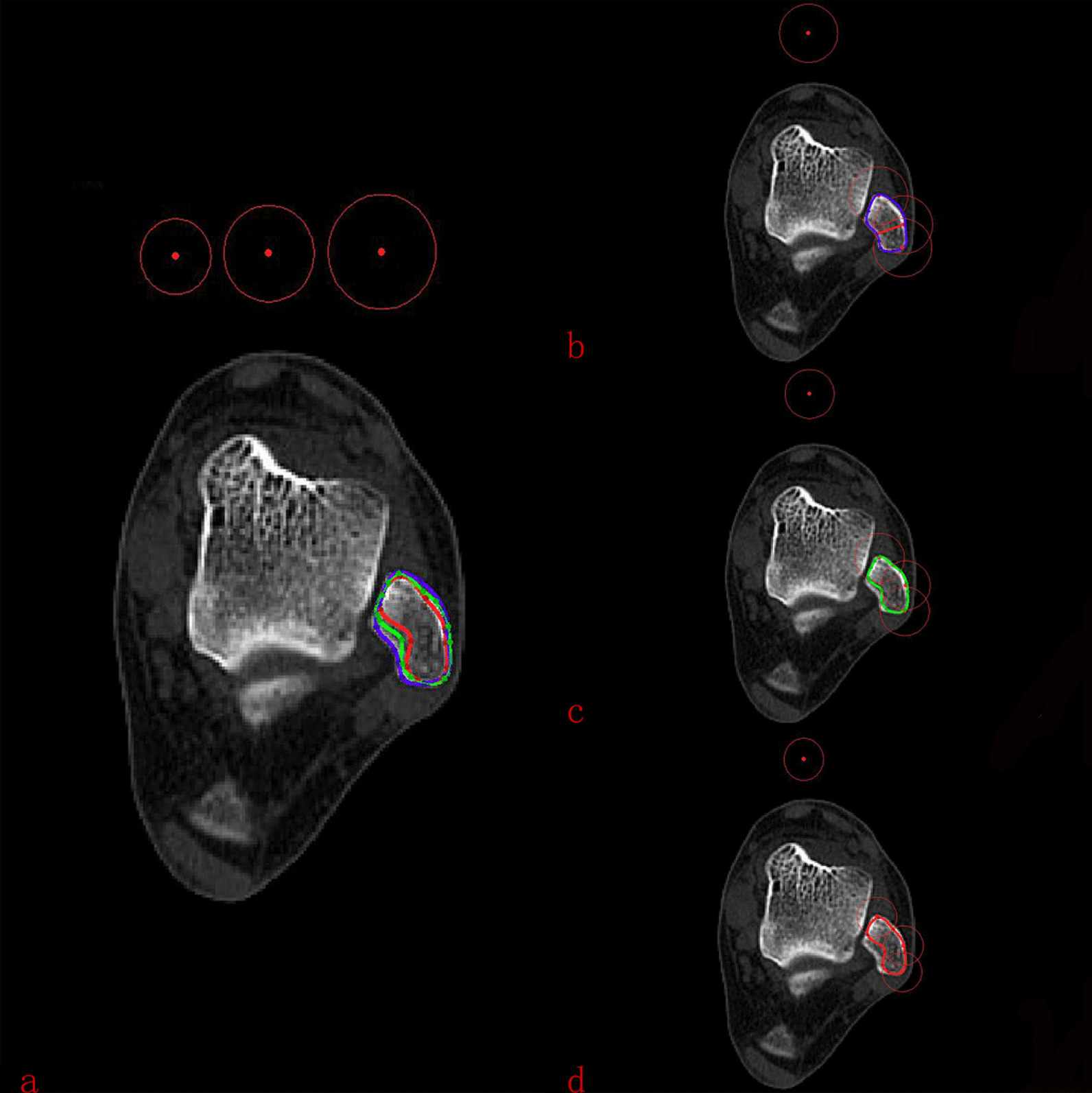
Methods: Anteroposterior CT reconstruction was performed on 248 subjects. After reconstruction, the deepest point of the lateral MF was located, and then, the cross-sectional shape of the lateral MF was observed and classified.
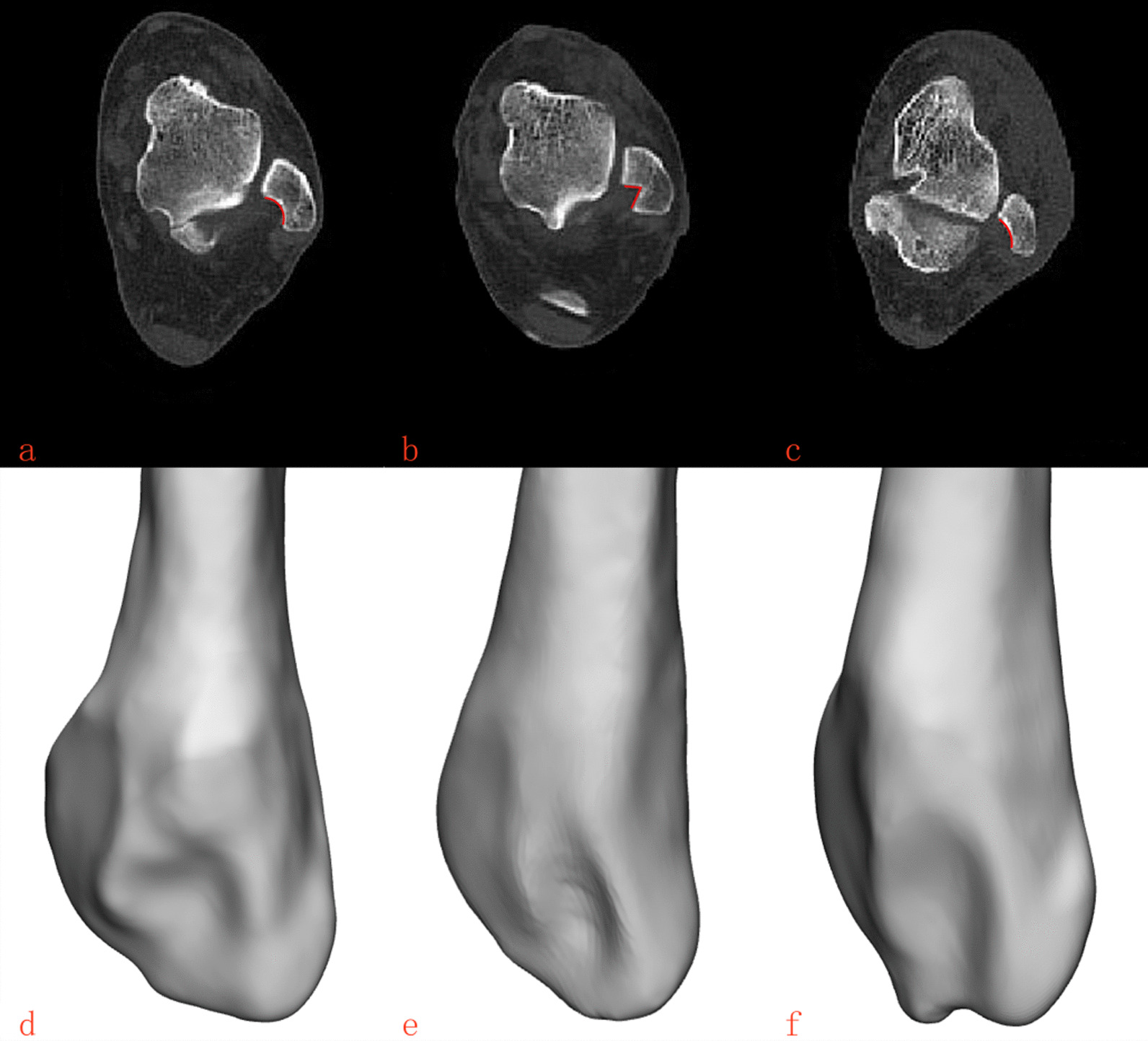
Results: According to the morphology of the CT cross section, the lateral MF was divided into three types: type C (43.1%), type V (32.2%), and type Flat (24.7%). Type V (3.98 ± 0.82) was significantly longer than type C(2.83 ± 0.54) and type Flat (1.84 ± 0.42) in cd. Similarly, in ∠α, Type Flat(136.31 ± 9.63) was the largest, followed by type C (116.51 ± 8.79), and type V (89.31 ± 9.07) was the smallest. Other measurements were not found any significant differences between the above.
Conclusion: According to the morphology of the CT cross section, the lateral MF was divided into three types: type C, type V and type Flat. Type V is most likely to be invaded when fixing the distal fibula. Screws less than 9 mm should be selected when fixing, and screws no more than 10 mm should be selected when there are type C and type Flat of MF.
Keywords: Ankle; Fibular fracture; Internal fixation; Lateral malleolar fossa.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare they have no competing interests. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this article.
Figures
Similar articles
-
Dimensions of the Lateral Malleolar Fossa and Its Potential Violation With Lateral Distal Fibular Plate Fixation.Orthopedics. 2020 May 1;43(3):e141-e146. doi: 10.3928/01477447-20200213-04. Epub 2020 Feb 20. Orthopedics. 2020. PMID: 32077963
-
Can CT-based assessment of lateral malleolus anatomy indicate when and how to perform an intramedullary fixation in distal fibula fractures? An analysis of 150 ankles.Eur J Orthop Surg Traumatol. 2023 Apr;33(3):601-609. doi: 10.1007/s00590-022-03360-6. Epub 2022 Aug 19. Eur J Orthop Surg Traumatol. 2023. PMID: 35984518
-
Nailing the fibula: alternative or standard treatment for lateral malleolar fracture fixation? A broken paradigm.Eur J Trauma Emerg Surg. 2021 Dec;47(6):1911-1920. doi: 10.1007/s00068-020-01337-w. Epub 2020 Mar 6. Eur J Trauma Emerg Surg. 2021. PMID: 32144445
-
Maisonneuve Fractures of the Ankle: A Critical Analysis Review.JBJS Rev. 2022 Feb 21;10(2). doi: 10.2106/JBJS.RVW.21.00160. JBJS Rev. 2022. PMID: 35180143 Review.
-
[Open reduction and internal fixation of posterior malleolus fractures].Oper Orthop Traumatol. 2021 Apr;33(2):112-124. doi: 10.1007/s00064-021-00705-y. Epub 2021 Mar 25. Oper Orthop Traumatol. 2021. PMID: 33765159 Review. German.
Cited by
-
Analysis of the effects of MIPPO under the anterolateral approach on stress indicators and ankle joint function in patients with open fracture of tibia and fibula.BMC Surg. 2025 Jul 3;25(1):273. doi: 10.1186/s12893-025-03030-4. BMC Surg. 2025. PMID: 40611190 Free PMC article.
References
-
- Gupton M, Munjal A, Kang M. Anatomy, bony pelvis and lower limb: fibula. In: StatPearls. Treasure Island: StatPearls Publishing; 2023.
MeSH terms
Grants and funding
- 82004458/National Natural Science Foundation of China (Youth Science Foundation Project)
- 2022-CXTD-08/Scientific Research Cultivation Project of The Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University
- 2022YFS0609/Supported by Sichuan Science and Technology Program
- 2022HJXNYD04/Hejiang People's Hospital - Southwest Medical University Science and Technology Strategic Cooperation Project
- 2023MS248./General Project of Sichuan Traditional Chinese Medicine Administration Traditional Chinese Medicine Research Special Project (Fundamentals of Traditional Chinese Medicine)
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
