Transdiagnostic subgroups of cognitive impairment in early affective and psychotic illness
- PMID: 37737273
- PMCID: PMC10789737
- DOI: 10.1038/s41386-023-01729-7
Transdiagnostic subgroups of cognitive impairment in early affective and psychotic illness
Abstract
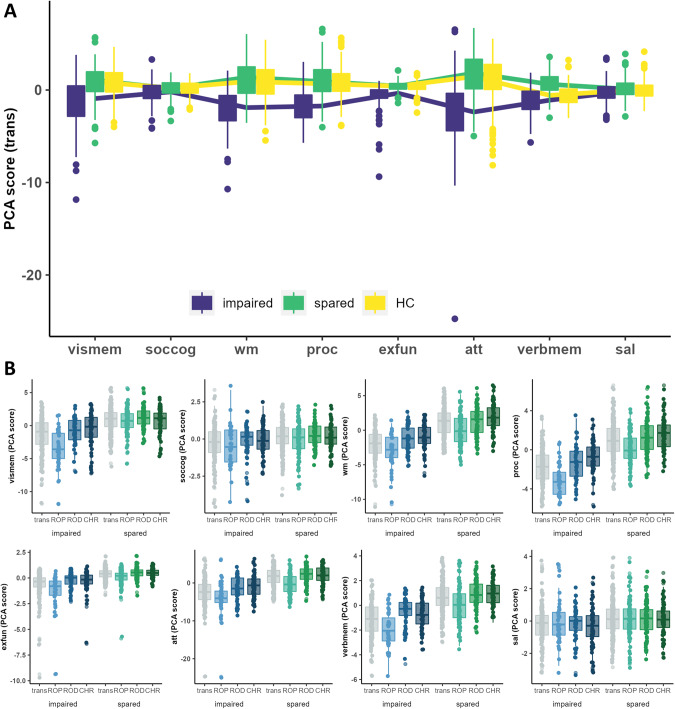
Cognitively impaired and spared patient subgroups were identified in psychosis and depression, and in clinical high-risk for psychosis (CHR). Studies suggest differences in underlying brain structural and functional characteristics. It is unclear whether cognitive subgroups are transdiagnostic phenomena in early stages of psychotic and affective disorder which can be validated on the neural level. Patients with recent-onset psychosis (ROP; N = 140; female = 54), recent-onset depression (ROD; N = 130; female = 73), CHR (N = 128; female = 61) and healthy controls (HC; N = 270; female = 165) were recruited through the multi-site study PRONIA. The transdiagnostic sample and individual study groups were clustered into subgroups based on their performance in eight cognitive domains and characterized by gray matter volume (sMRI) and resting-state functional connectivity (rsFC) using support vector machine (SVM) classification. We identified an impaired subgroup (NROP = 79, NROD = 30, NCHR = 37) showing cognitive impairment in executive functioning, working memory, processing speed and verbal learning (all p < 0.001). A spared subgroup (NROP = 61, NROD = 100, NCHR = 91) performed comparable to HC. Single-disease subgroups indicated that cognitive impairment is stronger pronounced in impaired ROP compared to impaired ROD and CHR. Subgroups in ROP and ROD showed specific symptom- and functioning-patterns. rsFC showed superior accuracy compared to sMRI in differentiating transdiagnostic subgroups from HC (BACimpaired = 58.5%; BACspared = 61.7%, both: p < 0.01). Cognitive findings were validated in the PRONIA replication sample (N = 409). Individual cognitive subgroups in ROP, ROD and CHR are more informative than transdiagnostic subgroups as they map onto individual cognitive impairment and specific functioning- and symptom-patterns which show limited overlap in sMRI and rsFC. CLINICAL TRIAL REGISTRY NAME: German Clinical Trials Register (DRKS). Clinical trial registry URL: https://www.drks.de/drks_web/ . Clinical trial registry number: DRKS00005042.
© 2023. The Author(s).
Conflict of interest statement
NK, JK, and RKRS are currently honorary speakers for Otsuka/Lundbeck. PAL has received honoraria for talks presented at educational meetings organised by Boehringer-Ingelheim. The remaining authors including members of the PRONIA consortium have nothing to disclose.
Figures