

Treatment of Ovarian Cancer Beyond PARP Inhibition: Current and Future Options
- PMID: 37737434
- PMCID: PMC10581945
- DOI: 10.1007/s40265-023-01934-0
Treatment of Ovarian Cancer Beyond PARP Inhibition: Current and Future Options
Abstract
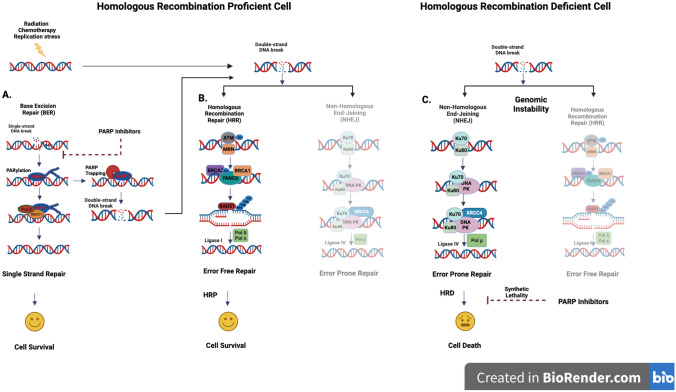
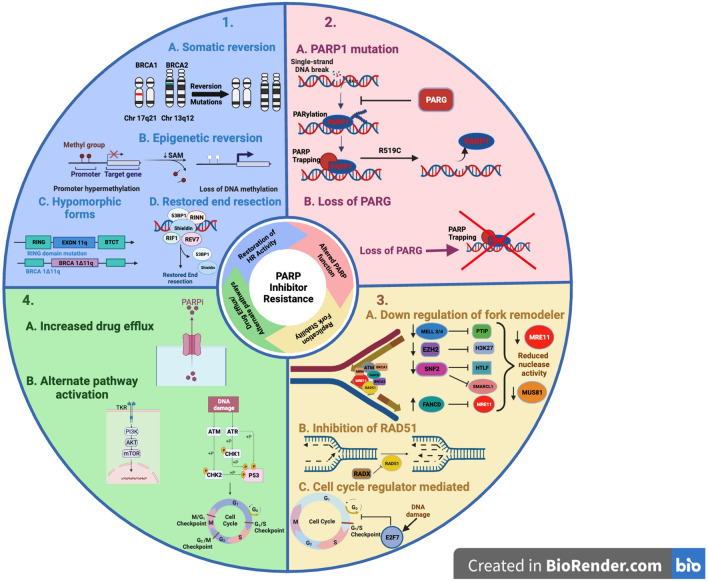
Ovarian cancer is the leading cause of gynecological cancer death. Improved understanding of the biologic pathways and introduction of poly (ADP-ribose) polymerase inhibitors (PARPi) during the last decade have changed the treatment landscape. This has improved outcomes, but unfortunately half the women with ovarian cancer still succumb to the disease within 5 years of diagnosis. Pathways of resistance to PARPi and chemotherapy have been studied extensively, but there is an unmet need to overcome treatment failure and improve outcome. Major mechanisms of PARPi resistance include restoration of homologous recombination repair activity, alteration of PARP function, stabilization of the replication fork, drug efflux, and activation of alternate pathways. These resistant mechanisms can be targeted to sensitize the resistant ovarian cancer cells either by rechallenging with PARPi, overcoming resistance mechanism or bypassing resistance pathways. Augmenting the PARPi activity by combining it with other targets in the DNA damage response pathway, antiangiogenic agents and immune checkpoint inhibitors can potentially overcome the resistance mechanisms. Methods to bypass resistance include targeting non-cross-resistant pathways acting independent of homologous recombination repair (HRR), modulating tumour microenvironment, and enhancing drug delivery systems such as antibody drug conjugates. In this review, we will discuss the first-line management of ovarian cancer, resistance mechanisms and potential strategies to overcome these.
© 2023. The Author(s).
Conflict of interest statement
Amit M. Oza: PI and Steering Committees with AstraZeneca and GSK; advisory boards for Merck (uncompensated) and Morphosys; and Chief Executive Officer at Ozmosis Research (uncompensated). Vikas Garg reports no conflicts of interest.
Figures

Similar articles
-
Repression of PFKFB3 sensitizes ovarian cancer to PARP inhibitors by impairing homologous recombination repair.Cell Commun Signal. 2025 Jan 25;23(1):48. doi: 10.1186/s12964-025-02056-8. Cell Commun Signal. 2025. PMID: 39863903 Free PMC article.
-
Overcoming PARPi resistance: Preclinical and clinical evidence in ovarian cancer.Drug Resist Updat. 2021 Mar;55:100744. doi: 10.1016/j.drup.2021.100744. Epub 2021 Jan 16. Drug Resist Updat. 2021. PMID: 33551306 Review.
-
The Clinical Challenges, Trials, and Errors of Combatting Poly(ADP-Ribose) Polymerase Inhibitors Resistance.Cancer J. 2021 Nov-Dec 01;27(6):491-500. doi: 10.1097/PPO.0000000000000562. Cancer J. 2021. PMID: 34904812 Free PMC article. Review.
-
PARP inhibitors in ovarian cancer: Mechanisms of resistance and implications to therapy.DNA Repair (Amst). 2025 May;149:103830. doi: 10.1016/j.dnarep.2025.103830. Epub 2025 Apr 3. DNA Repair (Amst). 2025. PMID: 40203475 Review.
-
PARP inhibitors in ovarian cancer: overcoming resistance with combination strategies.J Gynecol Oncol. 2022 May;33(3):e44. doi: 10.3802/jgo.2022.33.e44. Epub 2022 Mar 8. J Gynecol Oncol. 2022. PMID: 35320891 Free PMC article. Review.
Cited by
-
Tumor suppressor function of RBMS3 overexpression in EOC associated with immune cell infiltration.Heliyon. 2024 May 1;10(9):e30603. doi: 10.1016/j.heliyon.2024.e30603. eCollection 2024 May 15. Heliyon. 2024. PMID: 38726149 Free PMC article.
-
Genetic Polymorphisms in Base Excision Repair (BER) and Nucleotide Excision Repair (NER) Pathways as Potential Biomarkers for Gynecological Cancers: A Comprehensive Literature Review.Cancers (Basel). 2025 Jun 27;17(13):2170. doi: 10.3390/cancers17132170. Cancers (Basel). 2025. PMID: 40647471 Free PMC article. Review.
-
Progesterone Enhances Niraparib Efficacy in Ovarian Cancer by Promoting Palmitoleic-Acid-Mediated Ferroptosis.Research (Wash D C). 2024 May 24;7:0371. doi: 10.34133/research.0371. eCollection 2024. Research (Wash D C). 2024. PMID: 38798714 Free PMC article.
-
Elucidating the role of liver enzymes as markers and regulators in ovarian cancer: a synergistic approach using Mendelian randomization, single-cell analysis, and clinical evidence.Hum Genomics. 2024 Jun 24;18(1):71. doi: 10.1186/s40246-024-00642-4. Hum Genomics. 2024. PMID: 38915066 Free PMC article.
-
Advances and obstacles of T cell-based immunotherapy in gynecological malignancies.Mol Cancer. 2025 Jul 26;24(1):207. doi: 10.1186/s12943-025-02411-w. Mol Cancer. 2025. PMID: 40713697 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
