

An Intraoperative Telemedicine Program to Improve Perioperative Quality Measures: The ACTFAST-3 Randomized Clinical Trial
- PMID: 37738052
- PMCID: PMC10517374
- DOI: 10.1001/jamanetworkopen.2023.32517
An Intraoperative Telemedicine Program to Improve Perioperative Quality Measures: The ACTFAST-3 Randomized Clinical Trial
Abstract
Importance: Telemedicine for clinical decision support has been adopted in many health care settings, but its utility in improving intraoperative care has not been assessed.
Objective: To pilot the implementation of a real-time intraoperative telemedicine decision support program and evaluate whether it reduces postoperative hypothermia and hyperglycemia as well as other quality of care measures.
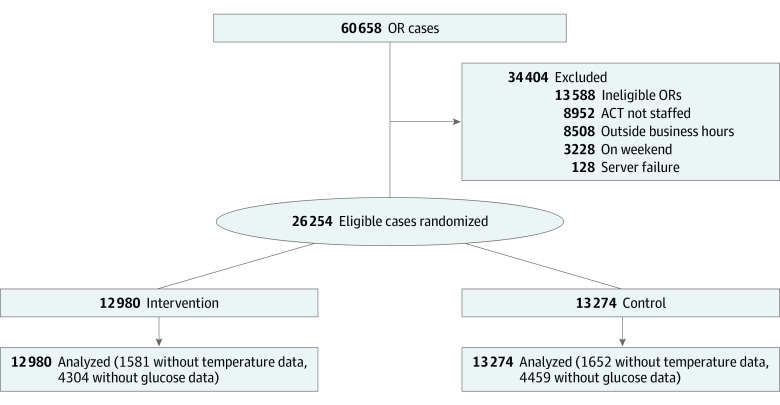
Design, setting, and participants: This single-center pilot randomized clinical trial (Anesthesiology Control Tower-Feedback Alerts to Supplement Treatments [ACTFAST-3]) was conducted from April 3, 2017, to June 30, 2019, at a large academic medical center in the US. A total of 26 254 adult surgical patients were randomized to receive either usual intraoperative care (control group; n = 12 980) or usual care augmented by telemedicine decision support (intervention group; n = 13 274). Data were initially analyzed from April 22 to May 19, 2021, with updates in November 2022 and February 2023.
Intervention: Patients received either usual care (medical direction from the anesthesia care team) or intraoperative anesthesia care monitored and augmented by decision support from the Anesthesiology Control Tower (ACT), a real-time, live telemedicine intervention. The ACT incorporated remote monitoring of operating rooms by a team of anesthesia clinicians with customized analysis software. The ACT reviewed alerts and electronic health record data to inform recommendations to operating room clinicians.
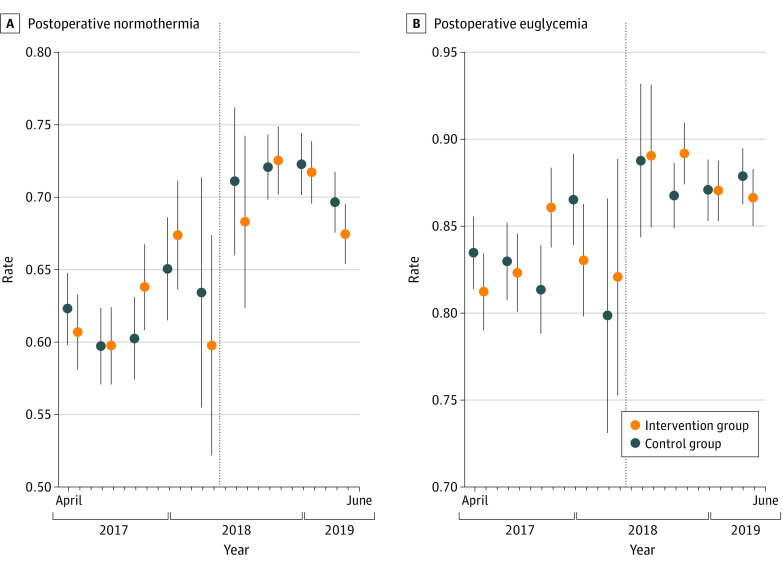
Main outcomes and measures: The primary outcomes were avoidance of postoperative hypothermia (defined as the proportion of patients with a final recorded intraoperative core temperature >36 °C) and hyperglycemia (defined as the proportion of patients with diabetes who had a blood glucose level ≤180 mg/dL on arrival to the postanesthesia recovery area). Secondary outcomes included intraoperative hypotension, temperature monitoring, timely antibiotic redosing, intraoperative glucose evaluation and management, neuromuscular blockade documentation, ventilator management, and volatile anesthetic overuse.
Results: Among 26 254 participants, 13 393 (51.0%) were female and 20 169 (76.8%) were White, with a median (IQR) age of 60 (47-69) years. There was no treatment effect on avoidance of hyperglycemia (7445 of 8676 patients [85.8%] in the intervention group vs 7559 of 8815 [85.8%] in the control group; rate ratio [RR], 1.00; 95% CI, 0.99-1.01) or hypothermia (7602 of 11 447 patients [66.4%] in the intervention group vs 7783 of 11 672 [66.7.%] in the control group; RR, 1.00; 95% CI, 0.97-1.02). Intraoperative glucose measurement was more common among patients with diabetes in the intervention group (RR, 1.07; 95% CI, 1.01-1.15), but other secondary outcomes were not significantly different.
Conclusions and relevance: In this randomized clinical trial, anesthesia care quality measures did not differ between groups, with high confidence in the findings. These results suggest that the intervention did not affect the targeted care practices. Further streamlining of clinical decision support and workflows may help the intraoperative telemedicine program achieve improvement in targeted clinical measures.
Trial registration: ClinicalTrials.gov Identifier: NCT02830126.
Conflict of interest statement
Figures
References
-
- WHO Group Consultation on Health Telematics . A health telematics policy in support of WHO’s health-for-all strategy for global health development. report of the WHO Group Consultation on Health Telematics, 11-16 December, Geneva, 1997. World Health Organization; 1998. Accessed March 5, 2023. https://apps.who.int/iris/bitstream/handle/10665/63857/WHO_DGO_98.1.pdf?...
-
- Mueller B. Telemedicine arrives in the UK: ‘10 years of change in one week’. New York Times. April 4, 2020. Accessed March 5, 2023. https://www.nytimes.com/2020/04/04/world/europe/telemedicine-uk-coronavi...
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
