

Aging-Related Mitochondrial Dysfunction Is Associated With Fibrosis in Benign Prostatic Hyperplasia
- PMID: 37738211
- PMCID: PMC11083627
- DOI: 10.1093/gerona/glad222
Aging-Related Mitochondrial Dysfunction Is Associated With Fibrosis in Benign Prostatic Hyperplasia
Abstract
Background: Age is the greatest risk factor for lower urinary tract symptoms attributed to benign prostatic hyperplasia (LUTS/BPH). Although LUTS/BPH can be managed with pharmacotherapy, treatment failure has been putatively attributed to numerous pathological features of BPH (eg, prostatic fibrosis, inflammation). Mitochondrial dysfunction is a hallmark of aging; however, its impact on the pathological features of BPH remains unknown.
Methods: Publicly available gene array data were analyzed. Immunohistochemistry examined mitochondrial proteins in the human prostate. The effect of complex I inhibition (rotenone) on a prostatic cell line was examined using quantitative polymerase chain reaction, immunocytochemistry, and Seahorse assays. Oleic acid (OA) was tested as a bypass of complex I inhibition. Aged mice were treated with OA to examine its effects on urinary dysfunction. Voiding was assessed longitudinally, and a critical complex I protein measured.
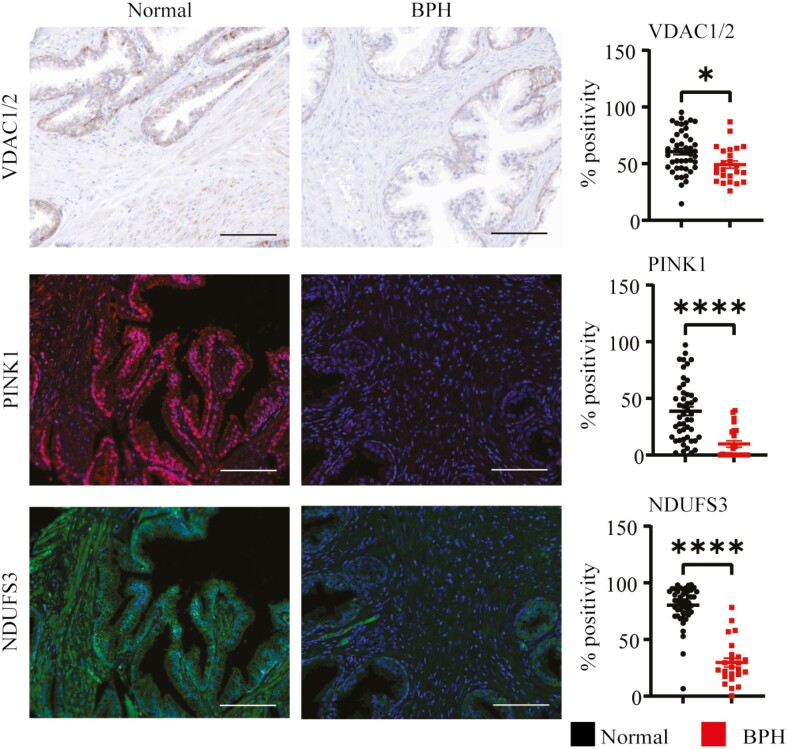
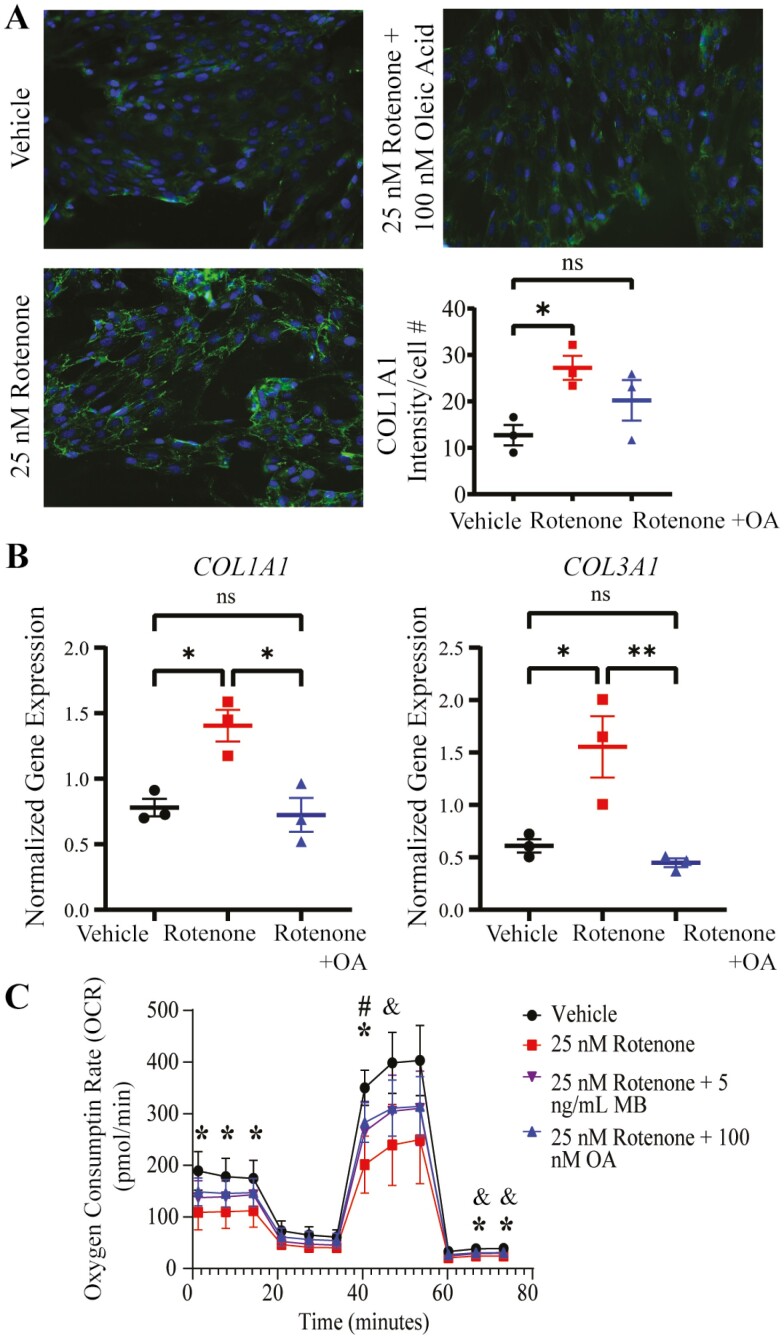
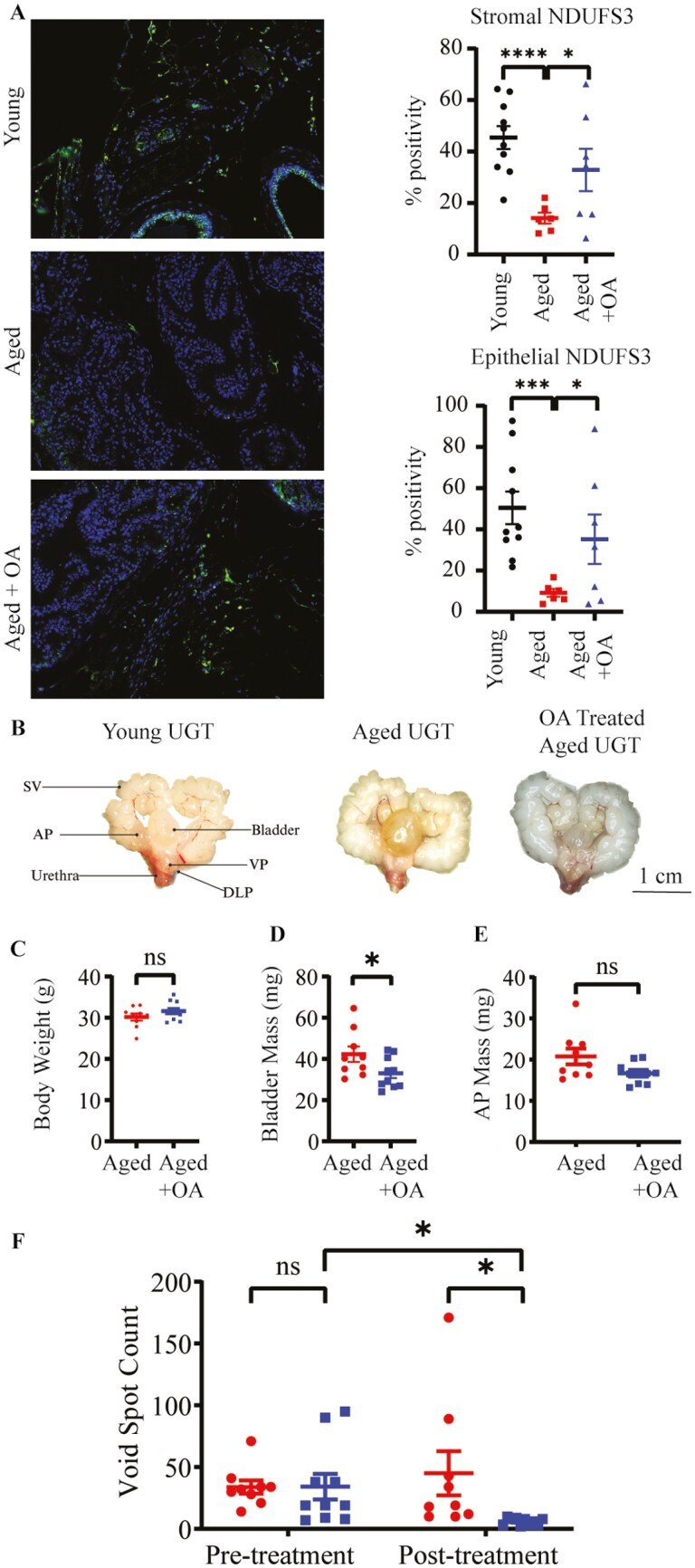
Results: Mitochondrial function and fibrosis genes were altered in BPH. Essential mitochondrial proteins (ie, voltage-dependent anion channels 1 and 2, PTEN-induced kinase 1, and NADH dehydrogenase [ubiquinone] iron-sulfur protein 3, mitochondrial [NDUFS3]) were significantly (p < .05) decreased in BPH. Complex I inhibition in cultured cells resulted in decreased respiration, altered NDUFS3 expression, increased collagen deposition, and gene expression. OA ameliorated these effects. OA-treated aged mice had significantly (p < .05) improved voiding function and higher prostatic NDUFS3 expression.
Conclusions: Complex I dysfunction is a potential contributor to fibrosis and lower urinary tract dysfunction in aged mice. OA partially bypasses complex I inhibition and therefore should be further investigated as a mitochondrial modulator for treatment of LUTS/BPH. Hypotheses generated in this investigation offer a heretofore unexplored cellular target of interest for the management of LUTS/BPH.
Keywords: Complex I; Lower urinary tract symptoms; Oxidative phosphorylation; Prostate; Urology.
© The Author(s) 2023. Published by Oxford University Press on behalf of The Gerontological Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
None.
Figures
References
-
- Jacobsen SJ, Jacobson DJ, Girman CJ, et al. Treatment for benign prostatic hyperplasia among community dwelling men: the Olmsted County Study of Urinary Symptoms and Health Status. J Urol. 1999;162:1301–1306. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- T32 GM141013/GM/NIGMS NIH HHS/United States
- P30 CA014520/CA/NCI NIH HHS/United States
- R01 DK135804/DK/NIDDK NIH HHS/United States
- R01 DK127081/DK/NIDDK NIH HHS/United States
- T32 GM141013/NH/NIH HHS/United States
- F31 DK136335/DK/NIDDK NIH HHS/United States
- K01 AG059899/AG/NIA NIH HHS/United States
- R03 AG067937/AG/NIA NIH HHS/United States
- K76 AG074903/AG/NIA NIH HHS/United States
- U54 DK104310/DK/NIDDK NIH HHS/United States
- R01 DK131175/DK/NIDDK NIH HHS/United States
- R01 DK127080/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
