

Health service readiness to provide care for HIV and cardiovascular disease risk factors in low- and middle-income countries
- PMID: 37738224
- PMCID: PMC10516419
- DOI: 10.1371/journal.pgph.0002373
Health service readiness to provide care for HIV and cardiovascular disease risk factors in low- and middle-income countries
Abstract
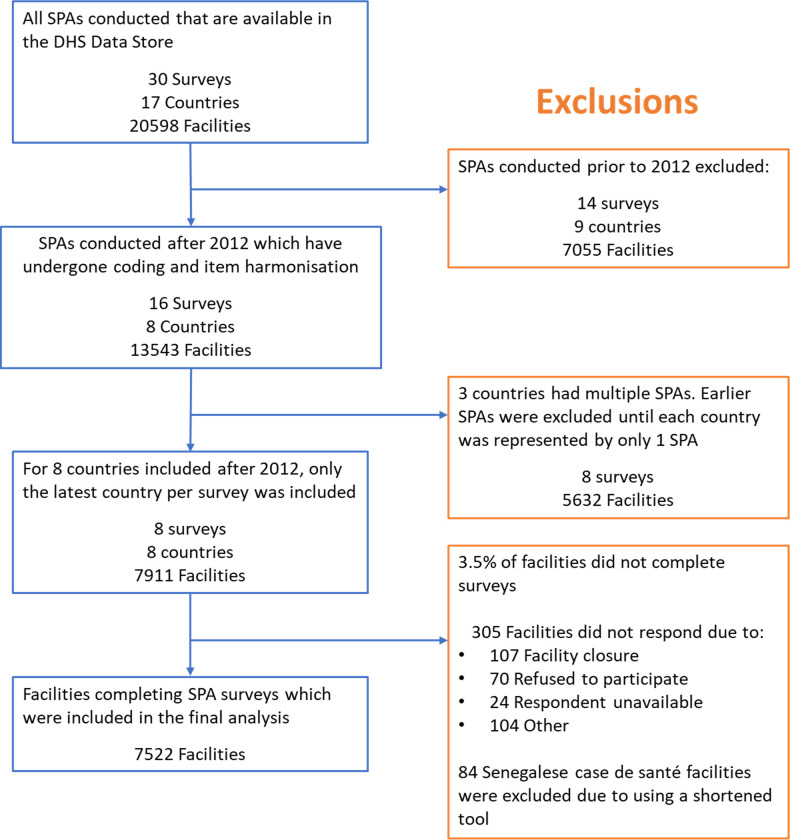
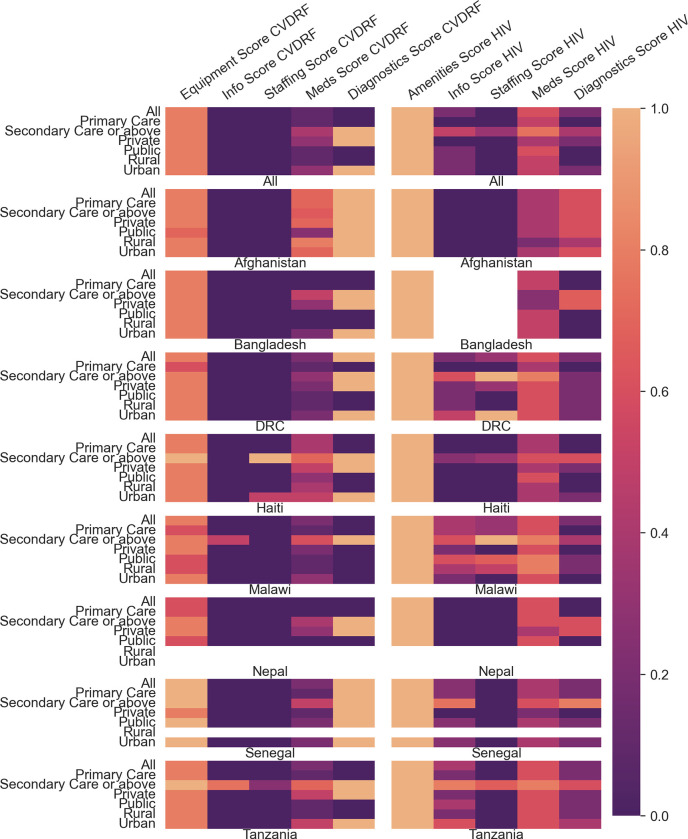
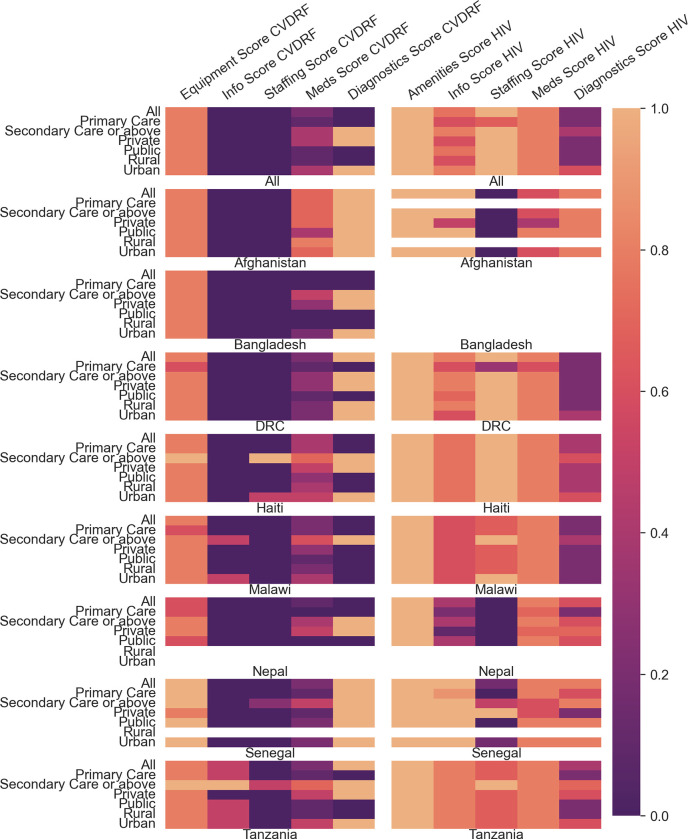
Cardiovascular disease risk factors (CVDRF), in particular diabetes and hypertension, are chronic conditions which carry a substantial disease burden in Low- and Middle-Income Countries. Unlike HIV, they were neglected in the Millenium Development Goals along with the health services required to manage them. To inform the level of health service readiness that could be achieved with increased attention, we compared readiness for CVDRF with that for HIV. Using data from national Service Provision Assessments, we describe facility-reported readiness to provide services for CVDRF and HIV, and derive a facility readiness score of observed essential components to manage them. We compared HIV vs CVDRF coverage scores by country, rural or urban location, and facility type, and by whether or not facilities reported readiness to provide care. We assessed the factors associated with coverage scores for CVDRF and HIV in a multivariable analysis. In our results, we include 7522 facilities in 8 countries; 86% of all facilities reported readiness to provide services for CVDRF, ranging from 77-98% in individual countries. For HIV, 30% reported of facilities readiness to provide services, ranging from 3-63%. Median derived facility readiness score for CVDRF was 0.28 (IQR 0.16-0.50), and for HIV was 0.43 (0.32-0.60). Among facilities which reported readiness, this rose to 0.34 (IQR 0.18-0.52) for CVD and 0.68 (0.56-0.76) for HIV. Derived readiness scores were generally significantly lower for CVDRF than for HIV, except in private facilities. In multivariable analysis, odds of a higher readiness score in both CVDRF or HIV care were higher in urban vs rural and secondary vs primary care; facilities with higher CVDRF scores were significantly associated with higher HIV scores. Derived readiness scores for HIV are higher than for CVDRF, and coverage for CVDRF is significantly higher in facilities with higher HIV readiness scores. This suggests possible benefits from leveraging HIV services to provide care for CVDRF, but poor coverage in rural and primary care facilities threatens Sustainable Development Goal 3.8 to provide high quality universal healthcare for all.
Copyright: © 2023 Cockburn et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Cardiovascular disease risk profile and management among people 40 years of age and above in Bo, Sierra Leone: A cross-sectional study.PLoS One. 2022 Sep 9;17(9):e0274242. doi: 10.1371/journal.pone.0274242. eCollection 2022. PLoS One. 2022. PMID: 36084117 Free PMC article.
-
Linking household and health facility surveys to assess obstetric service availability, readiness and coverage: evidence from 17 low- and middle-income countries.J Glob Health. 2018 Jun;8(1):010603. doi: 10.7189/jogh.08.010603. J Glob Health. 2018. PMID: 29862026 Free PMC article.
-
Health service readiness and quality for sick child care: an effective coverage analysis in eight low- and middle-income countries.J Glob Health. 2025 Apr 2;15:04085. doi: 10.7189/jogh.15.04085. J Glob Health. 2025. PMID: 40168517 Free PMC article.
-
Availability and readiness to provide sexually transmitted infections and HIV testing and counselling services in Nepal: evidence from comprehensive health facility survey.BMJ Open. 2020 Dec 15;10(12):e040918. doi: 10.1136/bmjopen-2020-040918. BMJ Open. 2020. PMID: 33323441 Free PMC article.
-
An analysis of health facility services readiness for non-communicable diseases in 8 LMICs in the universal health coverage era.Health Promot Perspect. 2024 Dec 30;14(4):343-349. doi: 10.34172/hpp.43175. eCollection 2024. Health Promot Perspect. 2024. PMID: 40041736 Free PMC article.
References
-
- Abbafati C, Abbas KM, Abbasi-Kangevari M, Abd-Allah F, Abdelalim A, Abdollahi M, et al.. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet 2020. Oct 17;396(10258):1204–22. Available from: http://www.thelancet.com/article/S0140673620309259/fulltext. doi: 10.1016/S0140-6736(20)30925-9 - DOI - PMC - PubMed
-
- Abbafati C, Abbas KM, Abbasi-Kangevari M, Abd-Allah F, Abdelalim A, Abdollahi M, et al.. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet. 2020. Oct 17;396(10258):1223–49. Available from: http://www.thelancet.com/article/S0140673620307522/fulltext. doi: 10.1016/S0140-6736(20)30752-2 - DOI - PMC - PubMed
-
- United Nations. THE 17 GOALS | Sustainable Development [Internet]. [cited 2022 Feb 16]. Available from: https://sdgs.un.org/goals.
-
- Flood D, Seiglie JA, Dunn M, Tschida S, Theilmann M, Marcus ME, et al.. The state of diabetes treatment coverage in 55 low-income and middle-income countries: a cross-sectional study of nationally representative, individual-level data in 680 102 adults. Lancet Healthy Longev. 2021. Jun 1;2(6):e340–51. doi: 10.1016/s2666-7568(21)00089-1 - DOI - PMC - PubMed
-
- Geldsetzer P, Manne-Goehler J, Marcus ME, Ebert C, Zhumadilov Z, Wesseh CS, et al.. The state of hypertension care in 44 low-income and middle-income countries: a cross-sectional study of nationally representative individual-level data from 1·1 million adults. The Lancet. 2019. Aug 24;394(10199):652–62. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0140673619309559. - PubMed
LinkOut - more resources
Full Text Sources