

Immune Monitoring-Guided Versus Fixed Duration of Antiviral Prophylaxis Against Cytomegalovirus in Solid-Organ Transplant Recipients: A Multicenter, Randomized Clinical Trial
- PMID: 37738676
- PMCID: PMC10874264
- DOI: 10.1093/cid/ciad575
Immune Monitoring-Guided Versus Fixed Duration of Antiviral Prophylaxis Against Cytomegalovirus in Solid-Organ Transplant Recipients: A Multicenter, Randomized Clinical Trial
Abstract
Background: The use of assays detecting cytomegalovirus (CMV)-specific T cell-mediated immunity may individualize the duration of antiviral prophylaxis after transplantation.
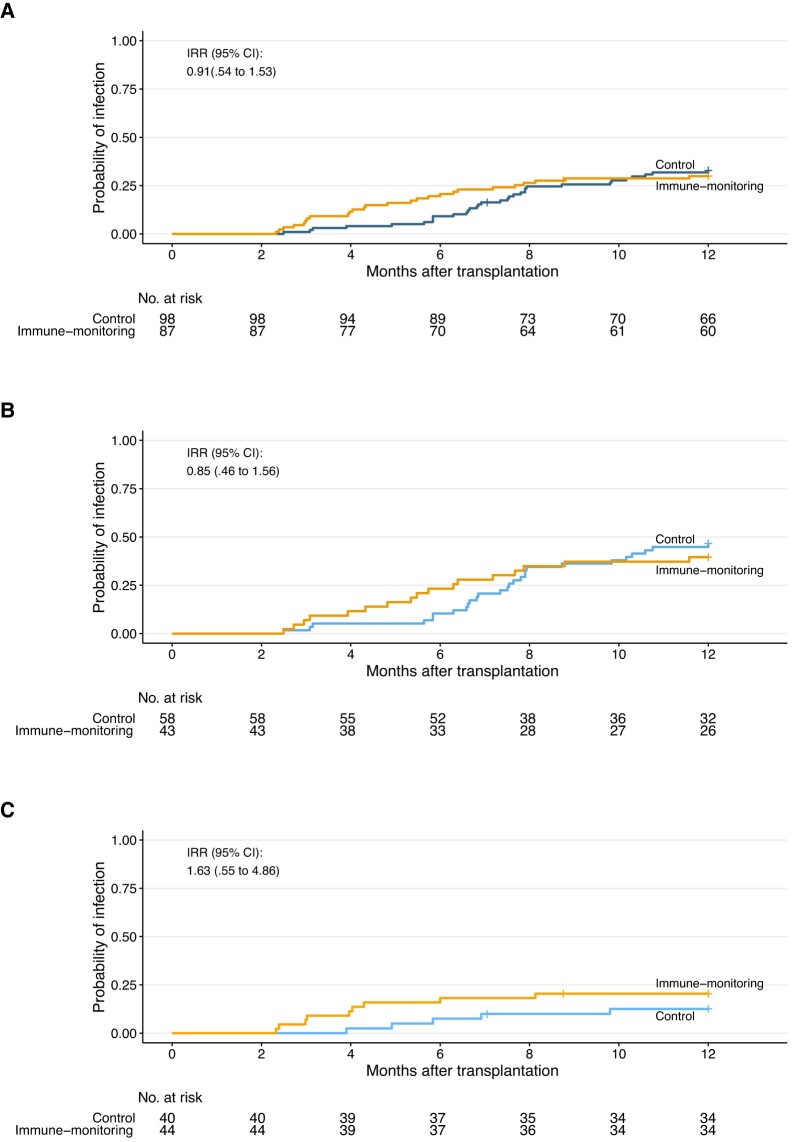
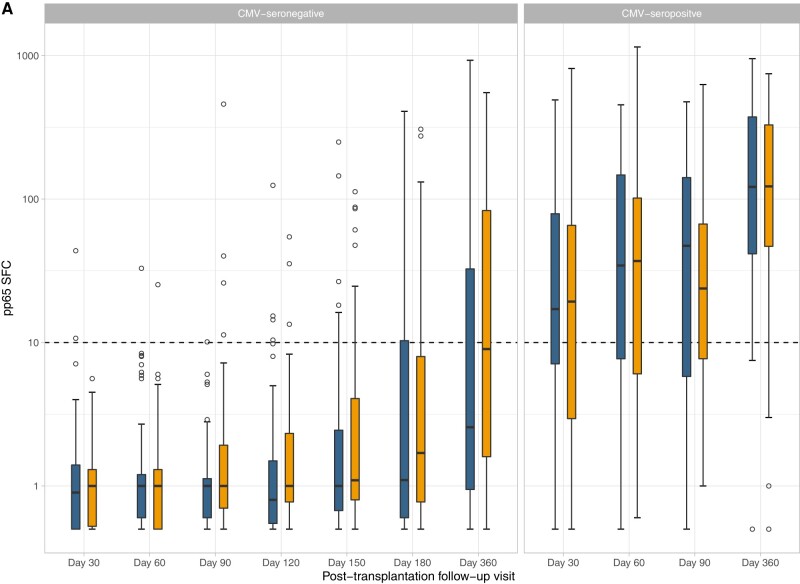
Methods: In this randomized trial, kidney and liver transplant recipients from 6 centers in Switzerland were enrolled if they were CMV-seronegative with seropositive donors or CMV-seropositive receiving antithymocyte globulins. Patients were randomized to a duration of antiviral prophylaxis based on immune monitoring (intervention) or a fixed duration (control). Patients in the control group were planned to receive 180 days (CMV-seronegative) or 90 days (CMV-seropositive) of valganciclovir. Patients were assessed monthly with a CMV ELISpot assay (T-Track CMV); prophylaxis in the intervention group was stopped if the assay was positive. The co-primary outcomes were the proportion of patients with clinically significant CMV infection and reduction in days of prophylaxis. Between-group differences were adjusted for CMV serostatus.
Results: Overall, 193 patients were randomized (92 in the immune-monitoring group and 101 in the control group), of whom 185 had evaluation of the primary outcome (87 and 98 patients). CMV infection occurred in 26 of 87 (adjusted percentage, 30.9%) in the immune-monitoring group and in 32 of 98 (adjusted percentage, 31.1%) in the control group (adjusted risk difference, -0.1; 95% confidence interval [CI], -13.0% to 12.7%; P = .064). The duration of prophylaxis was shorter in the immune-monitoring group (adjusted difference, -26.0 days; 95%, CI, -41.1 to -10.8 days; P < .001).
Conclusions: Immune monitoring resulted in a significant reduction of antiviral prophylaxis, but we were unable to establish noninferiority of this approach on the co-primary outcome of CMV infection.
Clinical trials registration: NCT02538172.
Keywords: cell-mediated immunity; personalized medicine; prevention; transplant; viral infection.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. O. M. reports research grants from Lophius Biosciences (acquired by Mikrogen), the Novartis Foundation, and the Swiss Transplant Cohort Study; participation on a data and safety monitoring board for Syneos and in advisory boards of MSD, Biotest, and Takeda; and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Takeda, paid to their institution. H. H. H. reports grants from Moderna paid to their institution; consulting fees from AiCuris, Allovir, Moderna, VeraTX, and Roche; and honoraria from VeraTX, Takeda, Biotest, and Gilead. P. J. reports serving as an unpaid member of the steering group of a trial funded by Terumo and research grants to their institution from Appili Therapeutics. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures




References
-
- Razonable RR, Humar A. Cytomegalovirus in solid organ transplant recipients—Guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant 2019; 33:e13512. - PubMed
-
- Lebranchu Y, Bridoux F, Buchler M, et al. Immunoprophylaxis with basiliximab compared with antithymocyte globulin in renal transplant patients receiving MMF-containing triple therapy. Am J Transplant 2002; 2:48–56. - PubMed
-
- Manuel O, Kralidis G, Mueller NJ, et al. Impact of antiviral preventive strategies on the incidence and outcomes of cytomegalovirus disease in solid organ transplant recipients. Am J Transplant 2013; 13:2402–10. - PubMed
-
- Kotton CN, Kumar D, Caliendo AM, et al. The third international consensus guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation 2018; 102:900–31. - PubMed
-
- Yong MK, Lewin SR, Manuel O. Immune monitoring for CMV in transplantation. Curr Infect Dis Rep 2018; 20:4. - PubMed
