

Subsite-specific metastatic organotropism and risk in gastric cancer: A population-based cohort study of the US SEER database and a Chinese single-institutional registry
- PMID: 37740601
- PMCID: PMC10587925
- DOI: 10.1002/cam4.6583
Subsite-specific metastatic organotropism and risk in gastric cancer: A population-based cohort study of the US SEER database and a Chinese single-institutional registry
Abstract
Background: Studies exploring whether metastatic organotropism and risk in gastric cancer (GC) differ by primary anatomical site are scarce.
Methods: This study included 15,260 and 1623 patients diagnosed with GC from the Surveillance, Epidemiology, and End Results (SEER) registry database and the Nanfang Hospital in China, respectively. Patients were stratified according to primary site of GC, and the incidence of metastasis to different organs was used to determine the metastatic organotropism for each GC subsite. Finally, the metastatic organotropism and risk were compared among the different subsite groups.
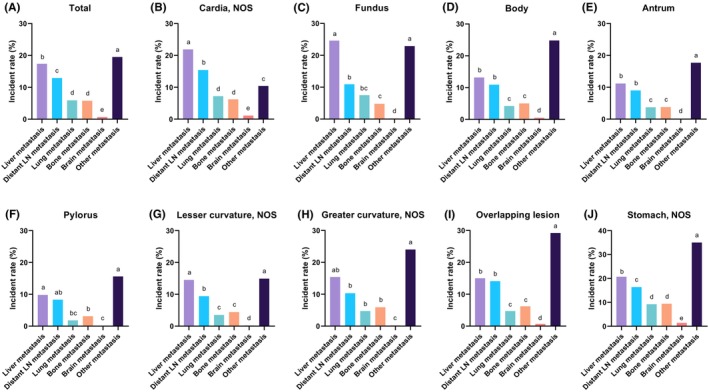
Results: Liver metastasis was the most common metastasis site in cardia GC, whereas other-site metastases were more common in the body, antrum, overlapping lesions, and unspecified GCs. Liver and other-site metastases were also frequently observed in the fundus, pylorus, lesser curvature, and greater curvature GCs. Patients with GC with definite primary tumor sites in the SEER and validation Nanfang hospital cohorts were compared by grouping as proximal and distal GCs for further analysis. In the SEER cohort, the top three metastatic sites of proximal GC were liver (21.4%), distant lymph node (LN) (14.6%), and other-site (mainly peritoneum, 11.9%), whereas those of distal GC were other-site (mainly peritoneum, 19.5%), liver (11.8%), and distant LN (9.5%). The incidence of metastasis to the liver, distant LN, lung, and brain was significantly higher in patients with proximal GC than in those with distal GC in both the SEER and Nanfang cohorts (p < 0.05). However, metastasis to other-site/peritoneum was significantly lower in patients with proximal GC compared to those with distal GC in the Nanfang Hospital and SEER cohorts, respectively (p < 0.05).
Conclusion: Liver and distant LN are the preferred metastatic sites for proximal GC, whereas peritoneal metastasis is more common in distal GC. Proximal GC has a higher risk of lymphatic and hematogenous metastases, and a lower risk of transcoelomic metastasis than distal GC. Our findings highlight the need to stratify GC by its primary subsite to aid in planning and decision-making related to metastatic management in clinical practice.
Keywords: gastric cancer; metastatic management; metastatic organotropism; metastatic risk; primary tumor location.
© 2023 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




Similar articles
-
Prognostic Value of the Site of Distant Metastasis and Surgical Interventions in Metastatic Gastric Cancer: A Population-Based Study.Technol Cancer Res Treat. 2020 Jan-Dec;19:1533033820964131. doi: 10.1177/1533033820964131. Technol Cancer Res Treat. 2020. PMID: 33111644 Free PMC article.
-
Frequency and clinicopathological features of metastasis to liver, lung, bone, and brain from gastric cancer: A SEER-based study.Cancer Med. 2018 Aug;7(8):3662-3672. doi: 10.1002/cam4.1661. Epub 2018 Jul 9. Cancer Med. 2018. PMID: 29984918 Free PMC article.
-
Sites of distant metastases and the cancer-specific survival of metastatic Siewert type II esophagogastric junction adenocarcinoma: a population-based study.Expert Rev Gastroenterol Hepatol. 2020 Jun;14(6):491-497. doi: 10.1080/17474124.2020.1760839. Epub 2020 Apr 29. Expert Rev Gastroenterol Hepatol. 2020. PMID: 32324423
-
20-Year Comparative Survival and Mortality of Cancer of the Stomach by Age, Sex, Race, Stage, Grade, Cohort Entry Time-Period, Disease Duration & Selected ICD-O-3 Oncologic Phenotypes: A Systematic Review of 157,258 Cases for Diagnosis Years 1973-2014: (SEER*Stat 8.3.4).J Insur Med. 2019;48(1):5-23. doi: 10.17849/insm-48-1-1-19.1. Epub 2019 Oct 14. J Insur Med. 2019. PMID: 31609640
-
Emerging evidence of the molecular landscape specific for hematogenous metastasis from gastric cancer.World J Gastrointest Oncol. 2018 Jun 15;10(6):124-136. doi: 10.4251/wjgo.v10.i6.124. World J Gastrointest Oncol. 2018. PMID: 29988904 Free PMC article. Review.
Cited by
-
Comprehensive analysis of risk factors and nomogram development for predicting hepatic metastasis following radical resection of adenocarcinoma of the esophagogastric junction.BMC Gastroenterol. 2025 May 27;25(1):409. doi: 10.1186/s12876-025-04014-7. BMC Gastroenterol. 2025. PMID: 40426037 Free PMC article.
-
Successful treatment with nivolumab in a patient with gastric cancer with severe liver failure resulting from multiple liver metastases: A case report.Oncol Lett. 2024 Apr 18;27(6):271. doi: 10.3892/ol.2024.14404. eCollection 2024 Jun. Oncol Lett. 2024. PMID: 38686354 Free PMC article.
-
Integrated single-cell RNA sequencing reveals the tumor heterogeneity and microenvironment landscape during liver metastasis in adenocarcinoma of esophagogastric junction.Front Immunol. 2025 Jan 9;15:1484234. doi: 10.3389/fimmu.2024.1484234. eCollection 2024. Front Immunol. 2025. PMID: 39850884 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209‐249. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
