

Interventions for reducing anticholinergic medication burden in older adults-a systematic review and meta-analysis
- PMID: 37740900
- PMCID: PMC10517713
- DOI: 10.1093/ageing/afad176
Interventions for reducing anticholinergic medication burden in older adults-a systematic review and meta-analysis
Abstract
Introduction: Anticholinergic medications block the neurotransmitter acetylcholine in the brain and peripheral nervous system. Many medications have anticholinergic properties, and the cumulative effect of these medications is termed anticholinergic burden. Increased anticholinergic burden can have short-term side effects such as dry mouth, blurred vision and urinary retention as well as long-term effects including dementia, worsening physical function and falls.
Methods: We carried out a systematic review (SR) with meta-analysis (MA) looking at randomised controlled trials addressing interventions to reduce anticholinergic burden in older adults.
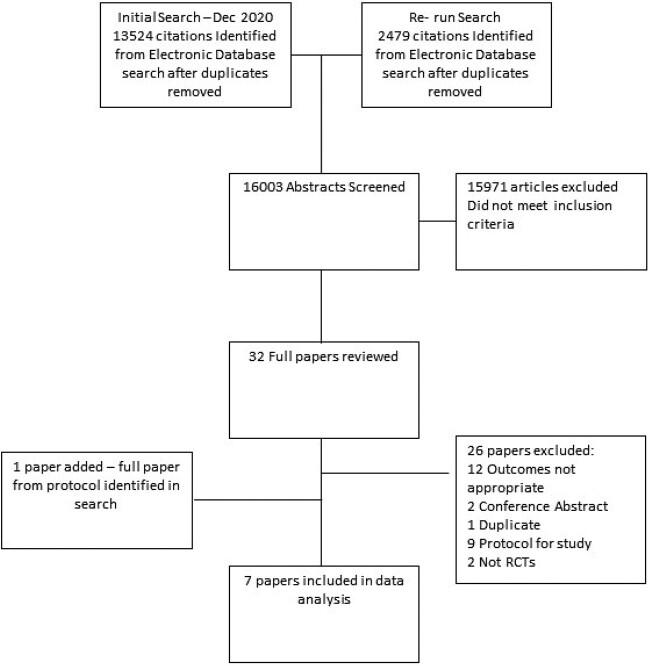
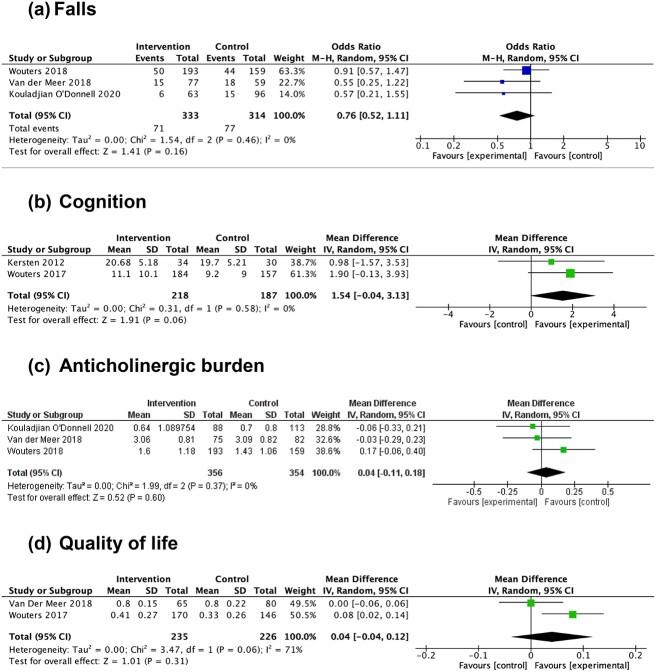
Results: We identified seven papers suitable for inclusion in our SR and MA. Interventions included multi-disciplinary involvement in medication reviews and deprescribing of AC medications. Pooled data revealed no significant difference in outcomes between control and intervention group for falls (OR = 0.76, 95% CI: 0.52-1.11, n = 647), cognition (mean difference = 1.54, 95% CI: -0.04 to 3.13, n = 405), anticholinergic burden (mean difference = 0.04, 95% CI: -0.11 to 0.18, n = 710) or quality of life (mean difference = 0.04, 95% CI: -0.04 to 0.12, n = 461).
Discussion: Overall, there was no significant difference with interventions to reduce anticholinergic burden. As we did not see a significant change in anticholinergic burden scores following interventions, it is likely other outcomes would not change. Short follow-up time and lack of training and support surrounding successful deprescribing may have contributed.
Keywords: anticholinergic medication; cognition; falls; meta-analysis; older adult; older people; systematic review.
© The Author(s) 2023. Published by Oxford University Press on behalf of the British Geriatrics Society. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
A.C. has led the development and validation of the Anticholinergic Medication Index (ACMI) in Health Data Research UK (HDR UK) funding. The ACMI will be supplied to UK providers of electronic health record systems and related software at no cost, on the basis that a premium charge is not applied to the end user. M.P. has received partnership funding for the following: MRC Clinical Pharmacology Training Scheme (co-funded by MRC and Roche, UCB, Eli Lilly and Novartis); and a PhD studentship jointly funded by EPSRC and Astra Zeneca. He has developed an HLA genotyping panel with MC Diagnostics, but does not benefit financially from this. He is part of the IMI Consortium ARDAT (
Figures
Similar articles
-
One-Year Evaluation of a Targeted Medication Therapy Management Intervention for Older Adults.J Manag Care Spec Pharm. 2020 Apr;26(4):520-528. doi: 10.18553/jmcp.2020.26.4.520. J Manag Care Spec Pharm. 2020. PMID: 32223601 Free PMC article.
-
Anticholinergic medications in patients admitted with cognitive impairment or falls (AMiCI). The impact of hospital admission on anticholinergic cognitive medication burden. Results of a multicentre observational study.J Clin Pharm Ther. 2018 Oct;43(5):682-694. doi: 10.1111/jcpt.12694. Epub 2018 May 4. J Clin Pharm Ther. 2018. PMID: 29729025
-
Deprescribing to reduce polypharmacy: study protocol for a randomised controlled trial assessing deprescribing of anticholinergic and sedative drugs in a cohort of frail older people living in the community.Trials. 2021 Nov 3;22(1):766. doi: 10.1186/s13063-021-05711-w. Trials. 2021. PMID: 34732234 Free PMC article.
-
Anticholinergic burden measures and older people's falls risk: a systematic prognostic review.Ther Adv Drug Saf. 2021 May 31;12:20420986211016645. doi: 10.1177/20420986211016645. eCollection 2021. Ther Adv Drug Saf. 2021. PMID: 34104401 Free PMC article. Review.
-
Anticholinergics and clinical outcomes amongst people with pre-existing dementia: A systematic review.Maturitas. 2021 Sep;151:1-14. doi: 10.1016/j.maturitas.2021.06.004. Epub 2021 Jun 20. Maturitas. 2021. PMID: 34446273
Cited by
-
Impact of cumulative exposure to anticholinergic and sedative drugs on cognition in older adults: a memory clinic cohort study.Alzheimers Res Ther. 2024 Jul 23;16(1):163. doi: 10.1186/s13195-024-01530-8. Alzheimers Res Ther. 2024. PMID: 39044289 Free PMC article.
-
Understanding the medication regimens associated with anticholinergic burden in older people's mental health services in the UK.BJPsych Open. 2024 Oct 3;10(5):e167. doi: 10.1192/bjo.2024.788. BJPsych Open. 2024. PMID: 39359152 Free PMC article.
-
Dual risk of anticholinergic burden and CSF alzheimer's biomarkers in older patients: a mortality follow-up study from daily medical practice.Alzheimers Res Ther. 2025 Jul 15;17(1):162. doi: 10.1186/s13195-025-01814-7. Alzheimers Res Ther. 2025. PMID: 40665403 Free PMC article.
-
The anticholinergic burden in patients with chronic kidney disease: Patterns, risk factors, and the link with cognitive impairment.J Am Geriatr Soc. 2025 Feb;73(2):533-544. doi: 10.1111/jgs.19283. Epub 2024 Nov 28. J Am Geriatr Soc. 2025. PMID: 39605299 Free PMC article.
-
Anticholinergic burden quantified using the Japanese risk scale as a predictor of frailty and sarcopenia among community-dwelling older adults: A 9-year Kashiwa cohort study.Geriatr Gerontol Int. 2025 Apr;25(4):520-527. doi: 10.1111/ggi.70012. Epub 2025 Mar 6. Geriatr Gerontol Int. 2025. PMID: 40047148 Free PMC article.
References
-
- Fox C, Smith T, Maidment Iet al. . Effect of medications with anti-cholinergic properties on cognitive function, delirium, physical function and mortality: a systematic review. Age Ageing 2014; 43: 604–15. - PubMed
-
- Landi F, Russo A, Liperoti Ret al. . Anticholinergic drugs and physical function among frail elderly population. Clin Pharmacol Ther 2007; 81: 235–41. - PubMed
-
- Nakham A, Myint PK, Bond CM, Newlands R, Loke YK, Cruickshank M. Interventions to reduce anticholinergic burden in adults aged 65 and older: a systematic review. J Am Med Dir Assoc 2020; 21: 172–180.e5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
