

An extraocular electrical stimulation approach to slow down the progression of retinal degeneration in an animal model
- PMID: 37741821
- PMCID: PMC10517961
- DOI: 10.1038/s41598-023-40547-1
An extraocular electrical stimulation approach to slow down the progression of retinal degeneration in an animal model
Erratum in
-
Author Correction: An extraocular electrical stimulation approach to slow down the progression of retinal degeneration in an animal model.Sci Rep. 2023 Oct 23;13(1):18120. doi: 10.1038/s41598-023-45262-5. Sci Rep. 2023. PMID: 37872269 Free PMC article. No abstract available.
Abstract
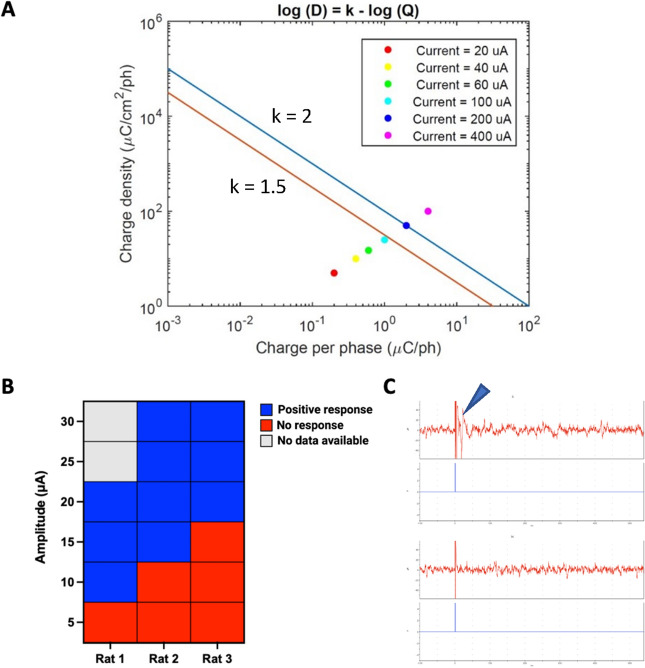
Retinal diseases such as retinitis pigmentosa (RP) and age-related macular degeneration (AMD) are characterized by unrelenting neuronal death. However, electrical stimulation has been shown to induce neuroprotective changes in the retina capable of slowing down the progression of retinal blindness. In this work, a multi-scale computational model and modeling platform were used to design electrical stimulation strategies to better target the bipolar cells (BCs), that along with photoreceptors are affected at the early stage of retinal degenerative diseases. Our computational findings revealed that biphasic stimulus pulses of long pulse duration could decrease the activation threshold of BCs, and the differential stimulus threshold between ganglion cells (RGCs) and BCs, offering the potential of targeting the BCs during the early phase of degeneration. In vivo experiments were performed to evaluate the electrode placement and parameters found to target bipolar cells and evaluate the safety and efficacy of the treatment. Results indicate that the proposed transcorneal Electrical Stimulation (TES) strategy can attenuate retinal degeneration in a Royal College of Surgeon (RCS) rodent model, offering the potential to translate this work to clinical practice.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
