

Machine learning-based analysis of regional differences in out-of-hospital cardiopulmonary arrest outcomes and resuscitation interventions in Japan
- PMID: 37741881
- PMCID: PMC10518013
- DOI: 10.1038/s41598-023-43210-x
Machine learning-based analysis of regional differences in out-of-hospital cardiopulmonary arrest outcomes and resuscitation interventions in Japan
Abstract
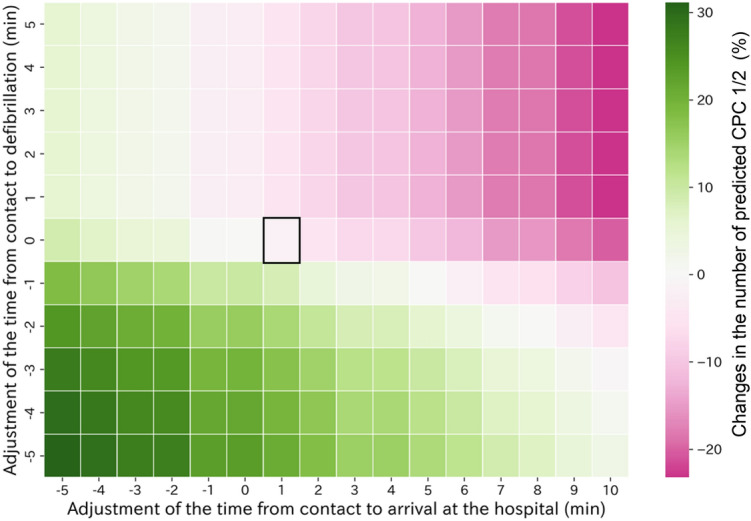
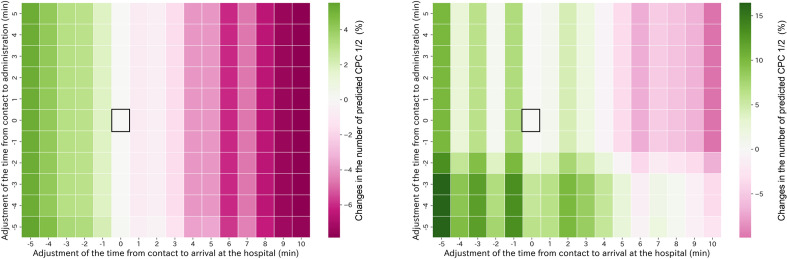
Refining out-of-hospital cardiopulmonary arrest (OHCA) resuscitation protocols for local emergency practices is vital. The lack of comprehensive evaluation methods for individualized protocols impedes targeted improvements. Thus, we employed machine learning to assess emergency medical service (EMS) records for examining regional disparities in time reduction strategies. In this retrospective study, we examined Japanese EMS records and neurological outcomes from 2015 to 2020 using nationwide data. We included patients aged ≥ 18 years with cardiogenic OHCA and visualized EMS activity time variations across prefectures. A five-layer neural network generated a neurological outcome predictive model that was trained on 80% of the data and tested on the remaining 20%. We evaluated interventions associated with changes in prognosis by simulating these changes after adjusting for time factors, including EMS contact to hospital arrival and initial defibrillation or drug administration. The study encompassed 460,540 patients, with the model's area under the curve and accuracy being 0.96 and 0.95, respectively. Reducing transport time and defibrillation improved outcomes universally, while combining transport time and drug administration showed varied efficacy. In conclusion, the association of emergency activity time with neurological outcomes varied across Japanese prefectures, suggesting the need to set targets for reducing activity time in localized emergency protocols.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
