

Targeting metacognitive change mechanisms in acute inpatients with psychotic symptoms: feasibility and acceptability of a modularized group intervention
- PMID: 37741946
- PMCID: PMC11127867
- DOI: 10.1007/s00406-023-01690-y
Targeting metacognitive change mechanisms in acute inpatients with psychotic symptoms: feasibility and acceptability of a modularized group intervention
Abstract
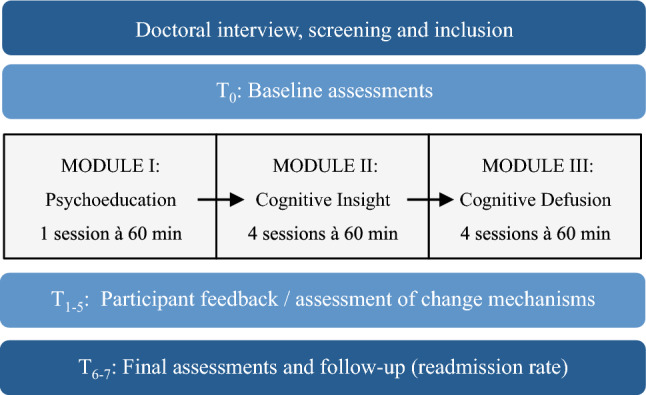
Emerging evidence suggests the usefulness of psychological interventions targeting metacognitive change mechanisms in patients experiencing psychosis. Although many of these patients are treated in acute psychiatric contexts, only few studies have adapted such interventions for acute inpatient settings. The present study aimed to assess the feasibility, acceptability, and preliminary clinical outcomes of a novel modularized group intervention focusing on different aspects of metacognitive change mechanisms. In particular, the intervention aims to reduce patients' acute symptoms by enhancing cognitive insight and to relieve distress via cognitive defusion (i.e. coping). A sample of 37 participants with acute psychosis received up to nine sessions of the intervention. Baseline and post-intervention assessments were conducted for general psychopathology, psychotic symptoms, global functioning, and symptom distress. Measures of change mechanisms were assessed before and after the respective treatment module. Participants' experiences were explored in feedback questionnaires and interviews. Recruitment, retention, and attendance rate met the pre-set feasibility benchmark of 80%. The intervention was well received by participants, who emphasised the group's clear structure, positive atmosphere, and helpful contents. Response rates were high and linear mixed models revealed significant medium-to-large time effects on all clinical outcomes. As expected, increase in hypothesised change mechanisms cognitive insight and decrease in cognitive fusion was found. However, the uncontrolled design limits interpreting clinical effects. The study provides evidence that an intervention based on a metacognitive model is feasible and acceptable for acute inpatients with psychosis. Positive results on clinical outcomes and change mechanisms warrant further exploration in a randomized controlled trial.
Keywords: Acute inpatient setting; Acute psychosis; Group therapy; Intervention; Mechanism-based; Metacognition; Modularized.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
