

Outcome of posterior decompression for spinal epidural lipomatosis
- PMID: 37743433
- PMCID: PMC10624717
- DOI: 10.1007/s00701-023-05814-0
Outcome of posterior decompression for spinal epidural lipomatosis
Abstract
Background: In contrast to osteoligamentous lumbar stenosis (LSS), outcome of surgical treatment for spinal epidural lipomatosis (SEL) is still not well defined. We present risk factors for SEL and clinical long-term outcome data after surgical treatment for patients with pure SEL and a mixed-type pathology with combined SEL and LSS (SEL+LSS) compared to patients with pure LSS.
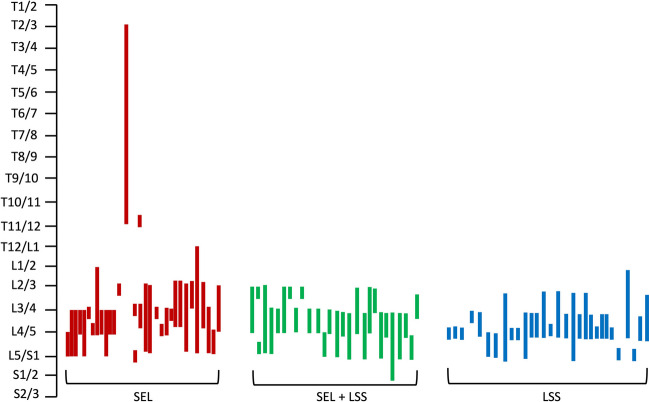
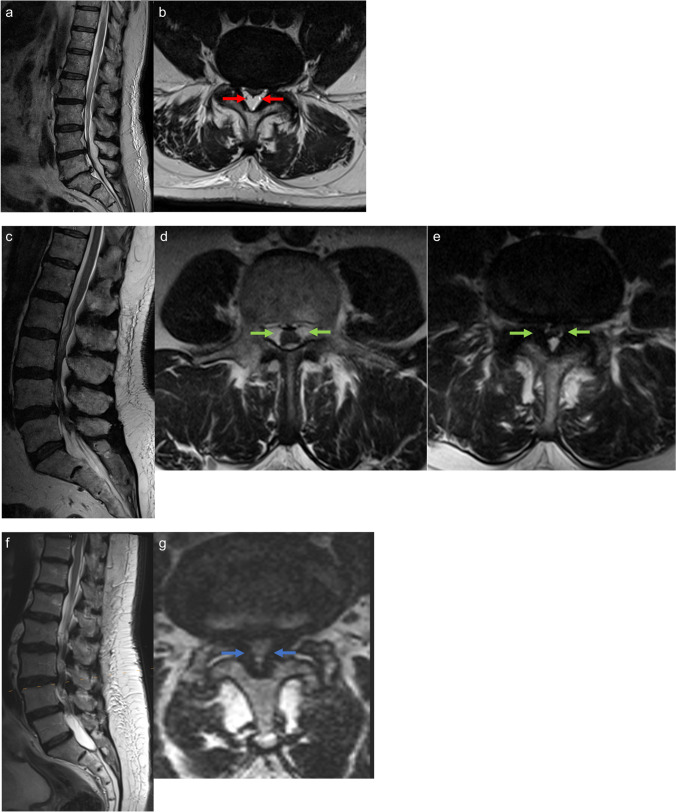
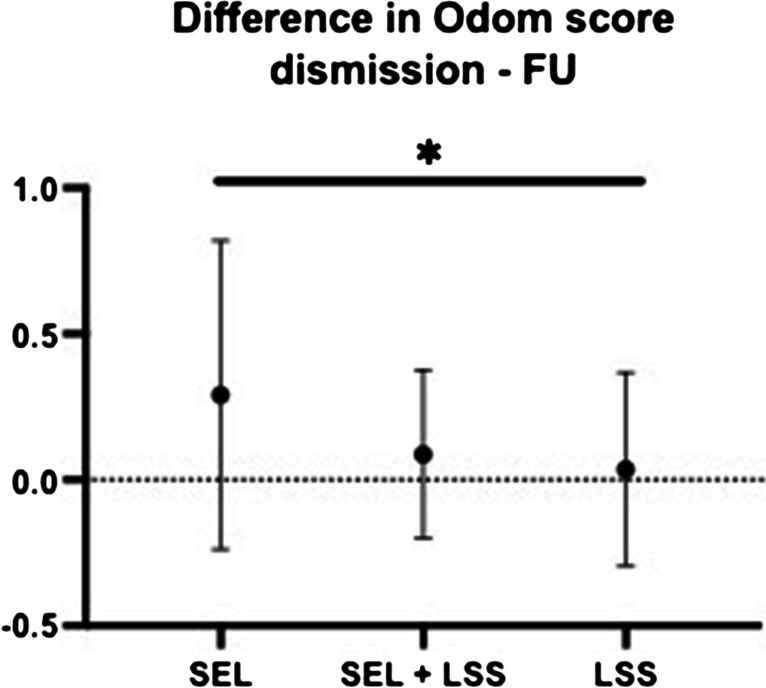
Methods: From our prospective institutional database, we identified all consecutive patients who were surgically treated for newly diagnosed SEL (n = 31) and SEL+LSS (n = 26) between 2018 and 2022. In addition, a matched control group of patients with pure LSS (n = 30) was compared. Microsurgical treatment aimed for posterior decompression of the spinal canal. Study endpoints were outcome data including clinical symptoms at presentation, MR-morphological analysis, evaluation of pain-free walking distance, pain perception by VAS-N/-R scales, and patient's satisfaction by determination of the Odom score.
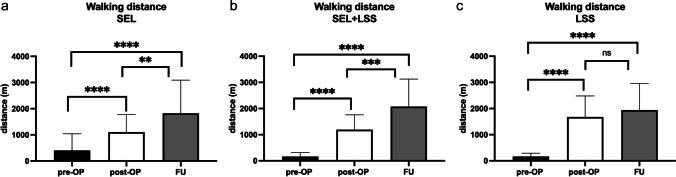
Results: Patients with osteoligamentous SEL were significantly more likely to suffer from obesity (body mass index (BMI) of 30.2 ± 5.5 kg/m2, p = 0.03), lumbar pain (p = 0.006), and to have received long-term steroid therapy (p = 0.01) compared to patients with SEL+LSS and LSS. In all three groups, posterior decompression of the spinal canal resulted in significant improvement of these symptoms. Patients with SEL had a significant increase in pain-free walking distance during the postoperative course, at discharge, and last follow-up (FU) (p < 0.0001), similar to patients with SEL+LSS and pure LSS. In addition, patients with pure SEL and SEL+LSS had a significant reduction in pain perception, represented by smaller values of VAS-N and -R postoperatively and at FU, similar to patients with pure LSS. In uni- and multivariate analysis, domination of lumbar pain and steroid long-term therapy were significant characteristic risk factors for SEL.
Conclusions: Surgical treatment of pure SEL and SEL+LSS allows significant improvement in pain-free walking distance and pain perception immediately postoperatively and in long-term FU, similar to patients with pure LSS.
Keywords: Posterior decompression; Spinal epidural lipomatosis; Spinal stenosis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
