

COVID-19 vaccine equity: a retrospective population-based cohort study examining primary series and first booster coverage among persons with a history of immigration and other residents of Ontario, Canada
- PMID: 37744516
- PMCID: PMC10515385
- DOI: 10.3389/fpubh.2023.1232507
COVID-19 vaccine equity: a retrospective population-based cohort study examining primary series and first booster coverage among persons with a history of immigration and other residents of Ontario, Canada
Abstract
Introduction: Immigrants were disproportionately impacted by COVID-19 and experience unique vaccination barriers. In Canada (37 million people), 23% of the population is foreign-born. Immigrants constitute 60% of the country's racialized (non-white) population and over half of immigrants reside in Ontario, the country's most populous province. Ontario had several strategies aimed at improving vaccine equity including geographic targeting of vaccine supply and clinics, as well as numerous community-led efforts. Our objectives were to (1) compare primary series vaccine coverage after it was widely available, and first booster coverage 6 months after its availability, between immigrants and other Ontario residents and (2) identify subgroups experiencing low coverage.
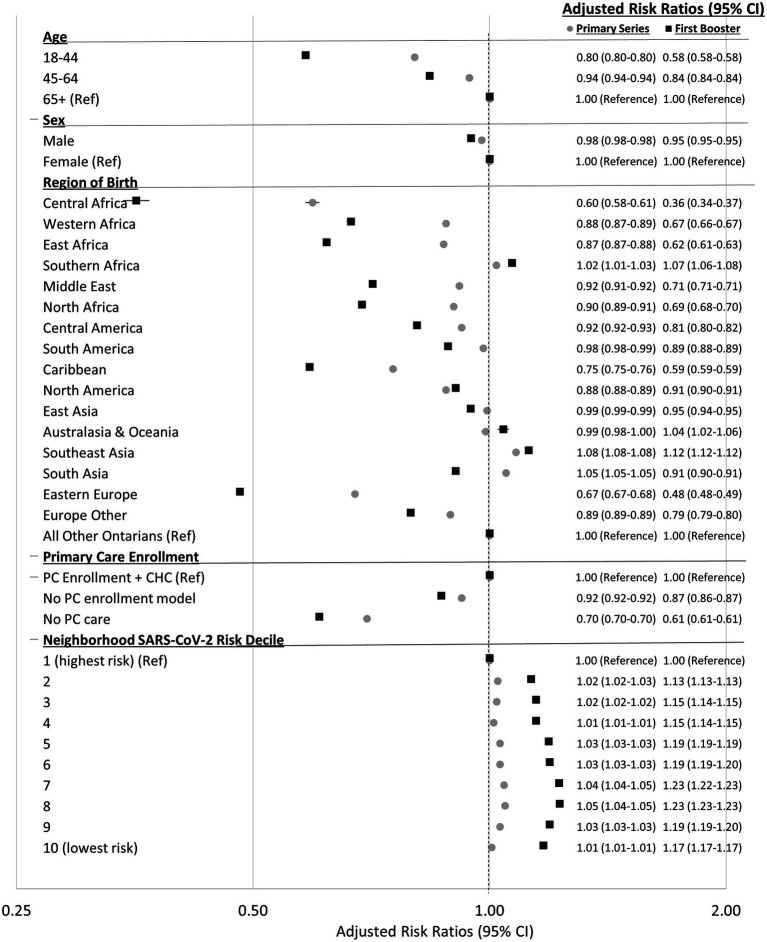
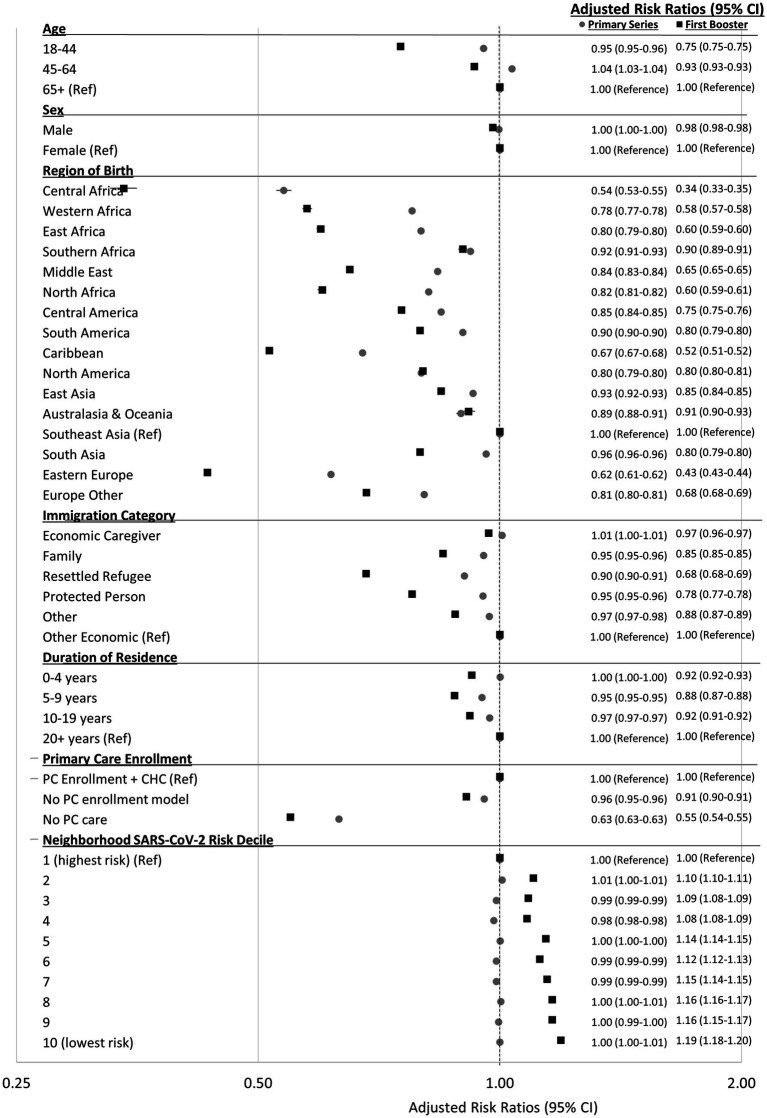
Materials and methods: Using linked immigration and health administrative data, we conducted a retrospective population-based cohort study including all community-dwelling adults in Ontario, Canada as of January 1, 2021. We compared primary series (two-dose) vaccine coverage by September 2021, and first booster (three-dose) coverage by March 2022 among immigrants and other Ontarians, and across sociodemographic and immigration characteristics. We used multivariable log-binomial regression to estimate adjusted risk ratios (aRR).
Results: Of 11,844,221 adults, 22% were immigrants. By September 2021, 72.6% of immigrants received two doses (vs. 76.4%, other Ontarians) and by March 2022 46.1% received three doses (vs. 58.2%). Across characteristics, two-dose coverage was similar or slightly lower, while three-dose coverage was much lower, among immigrants compared to other Ontarians. Across neighborhood SARS-CoV-2 risk deciles, differences in two-dose coverage were smaller in higher risk deciles and larger in the lower risk deciles; with larger differences across all deciles for three-dose coverage. Compared to other Ontarians, immigrants from Central Africa had the lowest two-dose (aRR = 0.60 [95% CI 0.58-0.61]) and three-dose coverage (aRR = 0.36 [95% CI 0.34-0.37]) followed by Eastern Europeans and Caribbeans, while Southeast Asians were more likely to receive both doses. Compared to economic immigrants, resettled refugees and successful asylum-claimants had the lowest three-dose coverage (aRR = 0.68 [95% CI 0.68-0.68] and aRR = 0.78 [95% CI 0.77-0.78], respectively).
Conclusion: Two dose coverage was more equitable than 3. Differences by immigrant region of birth were substantial. Community-engaged approaches should be re-invigorated to close gaps and promote the bivalent booster.
Keywords: COVID-19 vaccine; Ontario (Canada); immigrants; public health; refugees; social determinants of health.
Copyright © 2023 Wanigaratne, Lu, Gandhi, Shetty, Stukel, Piché-Renaud, Brandenberger, Abdi and Guttmann.
Conflict of interest statement
P-PP-R has been a co-investigator on an investigator-led project funded by Pfizer that is unrelated to this study. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Crawshaw AF, Farah Y, Deal A, Rustage K, Hayward SE, Carter J, et al. . Defining the determinants of vaccine uptake and undervaccination in migrant populations in Europe to improve routine and COVID-19 vaccine uptake: a systematic review. Lancet Infect Dis. (2022) 22:e254–66. doi: 10.1016/S1473-3099(22)00066-4, PMID: - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous