

Septic encephalopathy in the elderly - biomarkers of potential clinical utility
- PMID: 37744876
- PMCID: PMC10512712
- DOI: 10.3389/fncel.2023.1238149
Septic encephalopathy in the elderly - biomarkers of potential clinical utility
Abstract
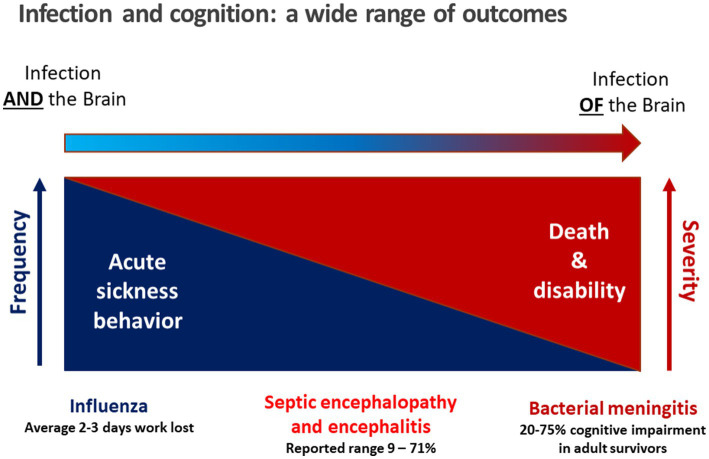
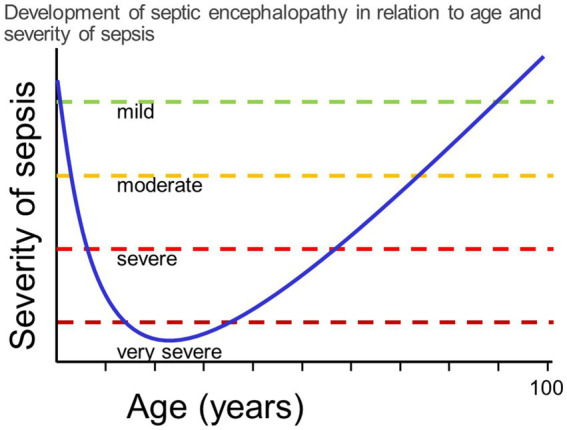
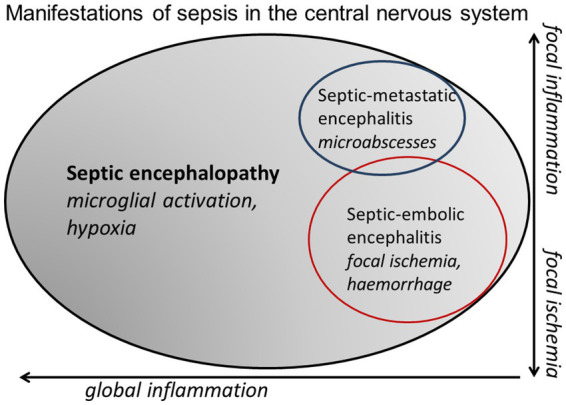
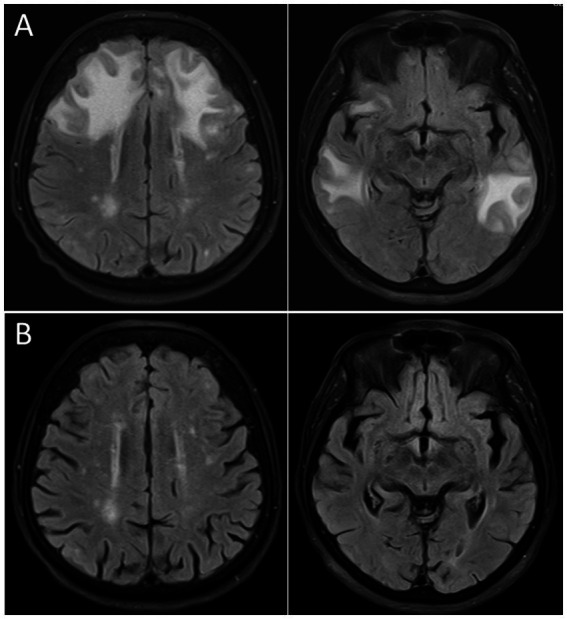
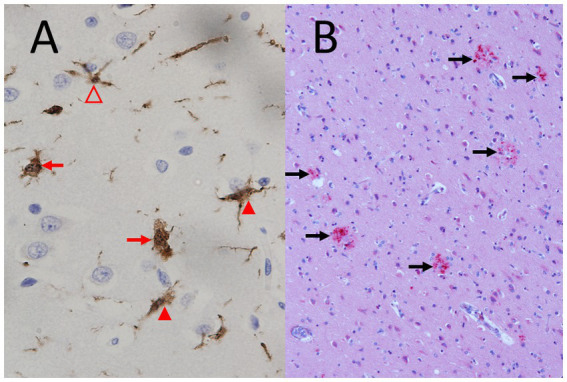
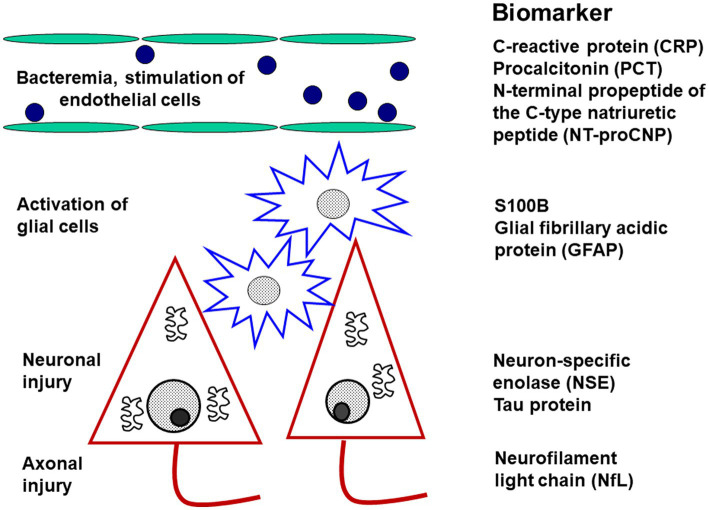
Next to acute sickness behavior, septic encephalopathy is the most frequent involvement of the brain during infection. It is characterized by a cross-talk of pro-inflammatory cells across the blood-brain barrier, by microglial activation and leukocyte migration, but not by the entry of infecting organisms into the brain tissue. Septic encephalopathy is very frequent in older persons because of their limited cognitive reserve. The predominant clinical manifestation is delirium, whereas focal neurological signs and symptoms are absent. Electroencephalography is a very sensitive method to detect functional abnormalities, but these abnormalities are not specific for septic encephalopathy and of limited prognostic value. Routine cerebral imaging by computer tomography usually fails to visualize the subtle abnormalities produced by septic involvement of the brain. Magnetic resonance imaging is by far more sensitive to detect vasogenic edema, diffuse axonal injury or small ischemic lesions. Routine laboratory parameters most suitable to monitor sepsis, but not specific for septic encephalopathy, are C-reactive protein and procalcitonin. The additional measurement of interleukin (IL)-6, IL-8, IL-10 and tumor necrosis factor-α increases the accuracy to predict delirium and an unfavorable outcome. The most promising laboratory parameters to quantify neuronal and axonal injury caused by septic encephalopathy are neurofilament light chains (NfL) and S100B protein. Neuron-specific enolase (NSE) plasma concentrations are strongly influenced by hemolysis. We propose to determine NSE only in non-hemolytic plasma or serum samples for the estimation of outcome in septic encephalopathy.
Keywords: S100B protein; cerebrospinal fluid; electroencephalography; magnetic resonance tomography; neurofilament light chains; plasma; positron emission tomography; sepsis.
Copyright © 2023 Schütze, Drevets, Tauber and Nau.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Diagnostic value of NT-proCNP compared to NSE and S100B in cerebrospinal fluid and plasma of patients with sepsis-associated encephalopathy.Neurosci Lett. 2019 Jan 23;692:167-173. doi: 10.1016/j.neulet.2018.11.014. Epub 2018 Nov 10. Neurosci Lett. 2019. PMID: 30423400
-
Sepsis-associated encephalopathy and septic encephalitis: an update.Expert Rev Anti Infect Ther. 2021 Feb;19(2):215-231. doi: 10.1080/14787210.2020.1812384. Epub 2020 Sep 14. Expert Rev Anti Infect Ther. 2021. PMID: 32808580 Review.
-
Translational evidence for two distinct patterns of neuroaxonal injury in sepsis: a longitudinal, prospective translational study.Crit Care. 2017 Oct 23;21(1):262. doi: 10.1186/s13054-017-1850-7. Crit Care. 2017. PMID: 29058589 Free PMC article.
-
Elevated serum levels of S-100beta protein and neuron-specific enolase are associated with brain injury in patients with severe sepsis and septic shock.Crit Care Med. 2006 Jul;34(7):1967-74. doi: 10.1097/01.CCM.0000217218.51381.49. Crit Care Med. 2006. PMID: 16607230
-
Treatment of septic encephalopathy and encephalitis - a critical appraisal.Expert Rev Neurother. 2023 Jul-Dec;23(12):1069-1080. doi: 10.1080/14737175.2023.2288652. Epub 2023 Dec 15. Expert Rev Neurother. 2023. PMID: 38019041 Review.
Cited by
-
Clinical image of sepsis-associated encephalopathy midst E. coli urosepsis: Emergency department database study.Heliyon. 2024 Apr 10;10(8):e29530. doi: 10.1016/j.heliyon.2024.e29530. eCollection 2024 Apr 30. Heliyon. 2024. PMID: 38655312 Free PMC article.
-
Modulation of brain immune microenvironment and cellular dynamics in systemic inflammation.Theranostics. 2025 Apr 9;15(11):5153-5171. doi: 10.7150/thno.107061. eCollection 2025. Theranostics. 2025. PMID: 40303348 Free PMC article.
-
Biomarker Profile in Peripheral Blood Cells Related to Alzheimer's Disease.Mol Neurobiol. 2025 Jul;62(7):8949-8964. doi: 10.1007/s12035-025-04767-y. Epub 2025 Mar 10. Mol Neurobiol. 2025. PMID: 40063315 Free PMC article.
-
The impact of sedation and analgesia scores on prognosis in critically ill sepsis patients with sepsis-associated encephalopathy: a retrospective analysis.Front Neurol. 2025 Jun 25;16:1622964. doi: 10.3389/fneur.2025.1622964. eCollection 2025. Front Neurol. 2025. PMID: 40635709 Free PMC article.
-
Essential New Complexity-Based Themes for Patient-Centered Diagnosis and Treatment of Dementia and Predementia in Older People: Multimorbidity and Multilevel Phenomenology.J Clin Med. 2024 Jul 18;13(14):4202. doi: 10.3390/jcm13144202. J Clin Med. 2024. PMID: 39064242 Free PMC article. Review.
References
-
- American Society for Psychiatry . (2022). Diagnostic and statistical manual of mental disorders, 5th edn, Text revision (DSM-5-TR. Washington, DC: American Society for Psychiatry.
-
- Anderson B. J., Reilly J. P., Shashaty M. G. S., Palakshappa J. A., Wysoczanski A., Dunn T. G., et al. . (2016). Admission plasma levels of the neuronal injury marker neuron-specific enolase are associated with mortality and delirium in sepsis. J. Crit. Care 36, 18–23. doi: 10.1016/j.jcrc.2016.06.012, PMID: - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous