

Systolic blood pressure ≤110 mm Hg is associated with severe coronary microvascular ischemia and higher risk for ventricular arrhythmias in hypertrophic cardiomyopathy
- PMID: 37744936
- PMCID: PMC10513918
- DOI: 10.1016/j.hroo.2023.07.009
Systolic blood pressure ≤110 mm Hg is associated with severe coronary microvascular ischemia and higher risk for ventricular arrhythmias in hypertrophic cardiomyopathy
Abstract
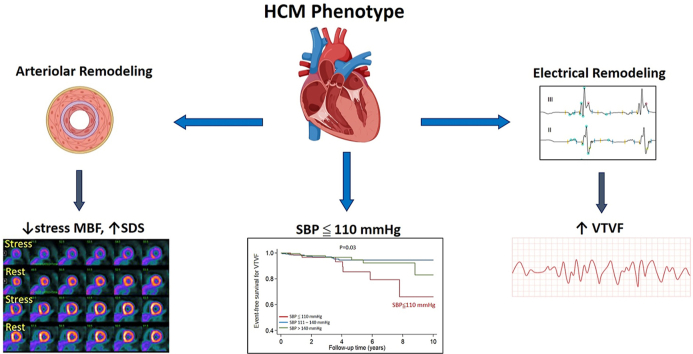
Background: Coronary microvascular dysfunction (CMD) and hypertension (HTN) occur frequently in hypertrophic cardiomyopathy (HCM), but whether blood pressure (BP) influences CMD and outcomes is unknown.
Objective: The purpose of this study was to test the hypothesis that HTN is associated with worse CMD and outcomes.
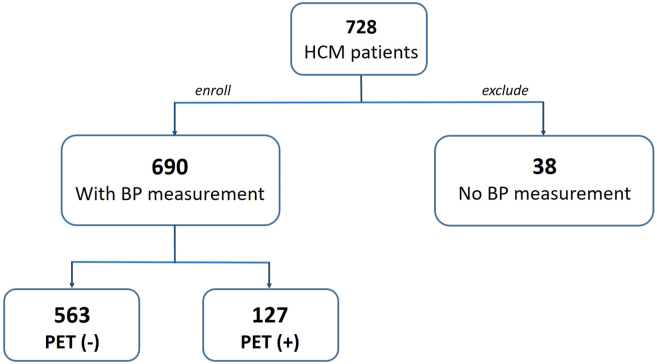
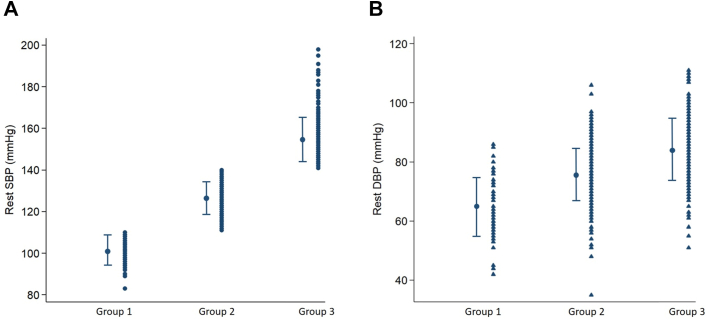
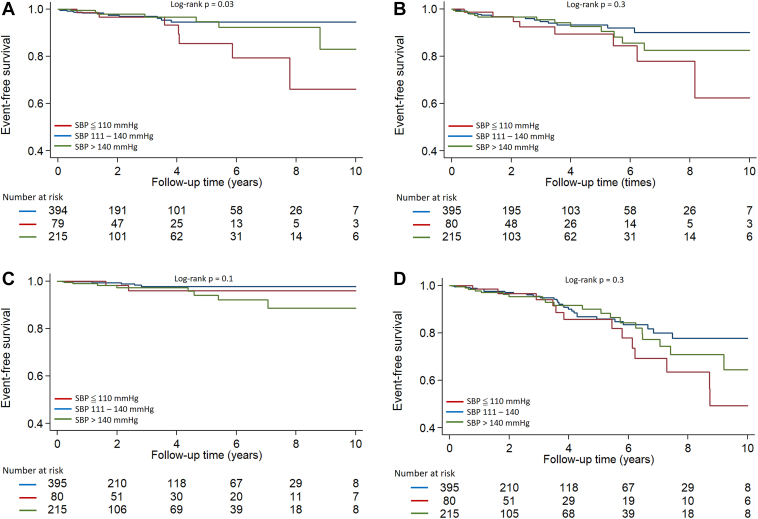
Methods: This retrospective study included 690 HCM patients. All patients underwent cardiac magnetic resonance imaging, echocardiography, and rhythm monitoring; 127 patients also underwent rest/vasodilator stress 13NH3 positron emission tomography myocardial perfusion imaging. Patients were divided into 3 groups based on their rest systolic blood pressure (SBP) (group 1 ≤110 mm Hg; group 2 111-140; group 3 >140 mm Hg) and were followed for development of ventricular tachycardia (VT)/ventricular fibrillation (VF), heart failure (HF), death, and composite outcome.
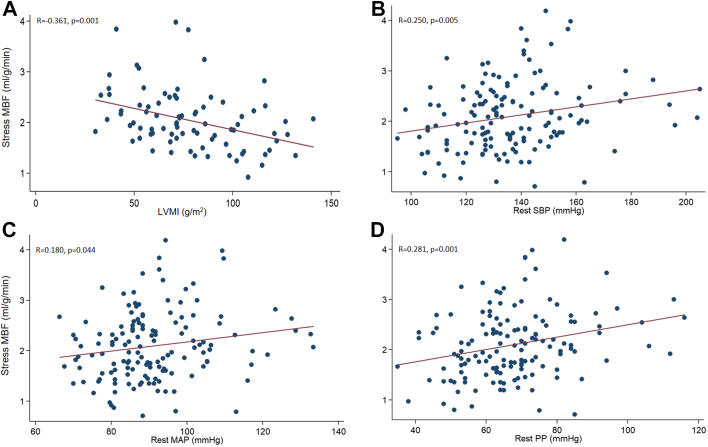
Results: Group 1 patients had the lowest age and left ventricular (LV) mass but the highest prevalence of nonobstructive hemodynamics and restrictive diastolic filling. LV scar was similar in the 3 groups. Group 1 had the lowest rest and stress myocardial blood flow (MBF) and highest SDS (summed difference score). Rest SBP was positively correlated with stress MBF and negatively correlated with SDS. Group 1 had the highest incidence of VT/VF, whereas the incidences of HF, death, and composite outcome were similar among the 3 groups. In multivariate analysis, rest SBP ≤110 mm Hg was independently associated with VT/VF (hazard ratio 2.6; 95% confidence interval 1.0-6.7; P = .04).
Conclusion: SBP ≤110 mm Hg is associated with greater severity of CMD and coronary microvascular ischemia and higher incidence of ventricular arrhythmias in HCM.
Keywords: Hypertrophic cardiomyopathy; Myocardial blood flow; Rest systolic blood pressure; Summed difference score; Ventricular fibrillation; Ventricular tachycardia.
© 2023 Published by Elsevier Inc. on behalf of Heart Rhythm Society.
Figures

Similar articles
-
Myocardial blood flow and left ventricular functional reserve in hypertrophic cardiomyopathy: a 13NH3 gated PET study.Eur J Nucl Med Mol Imaging. 2017 May;44(5):866-875. doi: 10.1007/s00259-016-3603-2. Epub 2017 Jan 3. Eur J Nucl Med Mol Imaging. 2017. PMID: 28050630
-
Higher incidence of vasodilator-induced left ventricular cavity dilation by PET when compared to treadmill exercise-ECHO in hypertrophic cardiomyopathy.J Nucl Cardiol. 2020 Dec;27(6):2031-2043. doi: 10.1007/s12350-018-01521-x. Epub 2018 Nov 19. J Nucl Cardiol. 2020. PMID: 30456498
-
Stress Myocardial Blood Flow Heterogeneity Is a Positron Emission Tomography Biomarker of Ventricular Arrhythmias in Patients With Hypertrophic Cardiomyopathy.Am J Cardiol. 2018 May 1;121(9):1081-1089. doi: 10.1016/j.amjcard.2018.01.022. Epub 2018 Feb 6. Am J Cardiol. 2018. PMID: 29678336 Free PMC article.
-
Clinical aspects of left ventricular diastolic function assessed by Doppler echocardiography following acute myocardial infarction.Dan Med Bull. 2001 Nov;48(4):199-210. Dan Med Bull. 2001. PMID: 11767125 Review.
-
Microvascular dysfunction, myocardial ischemia, and progression to heart failure in patients with hypertrophic cardiomyopathy.J Cardiovasc Transl Res. 2009 Dec;2(4):452-61. doi: 10.1007/s12265-009-9142-5. Epub 2009 Nov 3. J Cardiovasc Transl Res. 2009. PMID: 20560003 Review.
Cited by
-
Female predominance in nocturnal hypoxemia among elderly OSAS patients: hemoglobin mediates sex-specific hypoxic burden in Chinese cohorts.BMC Geriatr. 2025 Aug 7;25(1):598. doi: 10.1186/s12877-025-06281-1. BMC Geriatr. 2025. PMID: 40775746 Free PMC article.
References
-
- Ommen S.R., Mital S., Burke M.A., et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2020;76:e159–e240. - PubMed
-
- Maron B.J., Wolfson J.K., Epstein S.E., Roberts W.C. Intramural ("small vessel") coronary artery disease in hypertrophic cardiomyopathy. J Am Coll Cardiol. 1986;8:545–557. - PubMed
-
- Foa A., Agostini V., Rapezzi C., et al. Histopathological comparison of intramural coronary artery remodeling and myocardial fibrosis in obstructive versus end-stage hypertrophic cardiomyopathy. Int J Cardiol. 2019;291:77–82. - PubMed
-
- Gonzalez A., Ravassa S., Lopez B., et al. Myocardial remodeling in hypertension. Hypertension. 2018;72:549–558. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
