

Clinical phenotypes and outcomes in children with multisystem inflammatory syndrome across SARS-CoV-2 variant eras: a multinational study from the 4CE consortium
- PMID: 37745025
- PMCID: PMC10511777
- DOI: 10.1016/j.eclinm.2023.102212
Clinical phenotypes and outcomes in children with multisystem inflammatory syndrome across SARS-CoV-2 variant eras: a multinational study from the 4CE consortium
Abstract
Background: Multisystem inflammatory syndrome in children (MIS-C) is a severe complication of SARS-CoV-2 infection. It remains unclear how MIS-C phenotypes vary across SARS-CoV-2 variants. We aimed to investigate clinical characteristics and outcomes of MIS-C across SARS-CoV-2 eras.
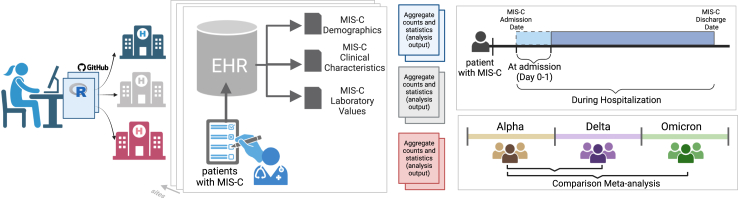
Methods: We performed a multicentre observational retrospective study including seven paediatric hospitals in four countries (France, Spain, U.K., and U.S.). All consecutive confirmed patients with MIS-C hospitalised between February 1st, 2020, and May 31st, 2022, were included. Electronic Health Records (EHR) data were used to calculate pooled risk differences (RD) and effect sizes (ES) at site level, using Alpha as reference. Meta-analysis was used to pool data across sites.
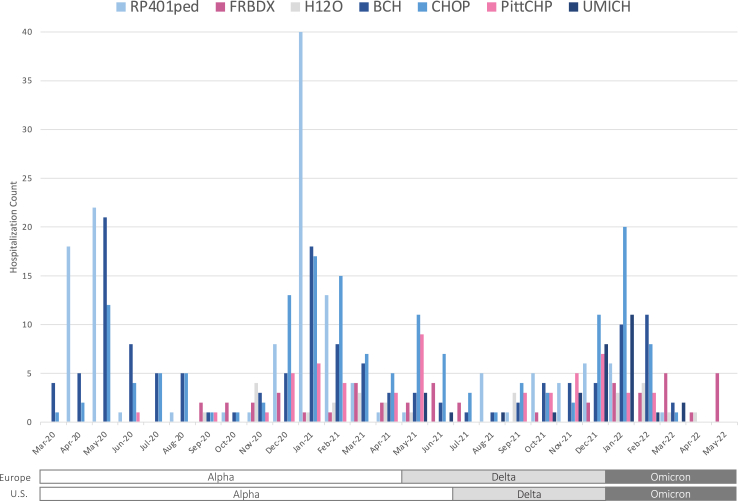
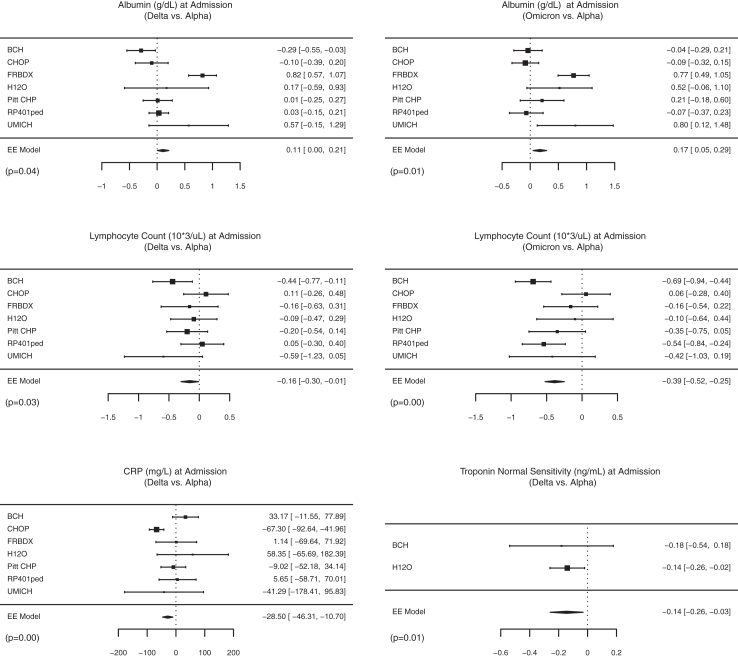
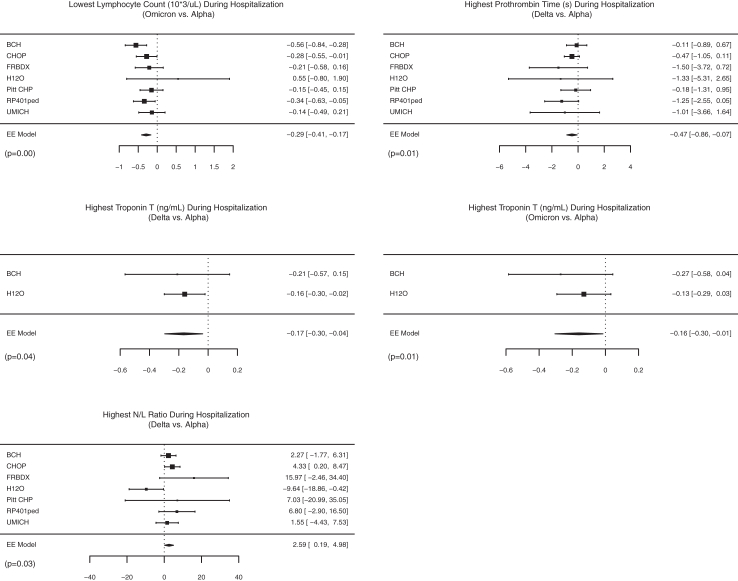
Findings: Of 598 patients with MIS-C (61% male, 39% female; mean age 9.7 years [SD 4.5]), 383 (64%) were admitted in the Alpha era, 111 (19%) in the Delta era, and 104 (17%) in the Omicron era. Compared with patients admitted in the Alpha era, those admitted in the Delta era were younger (ES -1.18 years [95% CI -2.05, -0.32]), had fewer respiratory symptoms (RD -0.15 [95% CI -0.33, -0.04]), less frequent non-cardiogenic shock or systemic inflammatory response syndrome (SIRS) (RD -0.35 [95% CI -0.64, -0.07]), lower lymphocyte count (ES -0.16 × 109/uL [95% CI -0.30, -0.01]), lower C-reactive protein (ES -28.5 mg/L [95% CI -46.3, -10.7]), and lower troponin (ES -0.14 ng/mL [95% CI -0.26, -0.03]). Patients admitted in the Omicron versus Alpha eras were younger (ES -1.6 years [95% CI -2.5, -0.8]), had less frequent SIRS (RD -0.18 [95% CI -0.30, -0.05]), lower lymphocyte count (ES -0.39 × 109/uL [95% CI -0.52, -0.25]), lower troponin (ES -0.16 ng/mL [95% CI -0.30, -0.01]) and less frequently received anticoagulation therapy (RD -0.19 [95% CI -0.37, -0.04]). Length of hospitalization was shorter in the Delta versus Alpha eras (-1.3 days [95% CI -2.3, -0.4]).
Interpretation: Our study suggested that MIS-C clinical phenotypes varied across SARS-CoV-2 eras, with patients in Delta and Omicron eras being younger and less sick. EHR data can be effectively leveraged to identify rare complications of pandemic diseases and their variation over time.
Funding: None.
Keywords: COVID-19; Clinical phenotypes; Multisystem inflammatory syndrome; Outcomes; Paediatric inflammatory multisystem syndrome; Pediatrics; SARS-CoV-2; Variants.
© 2023 The Authors.
Conflict of interest statement
The authors have no conflicts of interests to declare related to the content of this manuscript. JNW has research grant funding from National Heart, Lung, and Blood Institute (NHLBI), the Department of Defense, the Centres for Disease Control (CDC), and Pfizer; has been a consultant for Pfizer; chaired the Independent Events Adjudication Committees for Novartis, Pfizer, and Bristol-Myer-Squibb; and received honoraria from Daiichi Sankyo for service on the Steering Committee of the ENNOBLE-ATE Trial and from UpToDate. GSO has research grant funding from the National Institute of Environmental Health Sciences (NIEHS), National Institutes of Health (NIH), and from the National Cancer Institute (NCI). DAH has research grant funding from the National Center for Advancing Translational Sciences (NCATS). TGG has research grant funding from the Institute of Health Carlos III, the European Regional Development Fund (ERDF), the National Institute of Environmental Health Sciences (NIEHS), National Institutes of Health (NIH), and National Cancer Institute (NCI). KFK has research grant funding from the National Institute of Child Health and Human Development (NIHCD). SEM has research grant funding from the National Center for Advancing Translational Sciences (NCATS). AD has research grant funding from Pfizer. DMT has research grant funding from NIH. AMS has research grant funding from the National Heart, Lung, and Blood Institute (NHLBI) and from the National Center for Advancing Translational Sciences (NCATS). GV has internal research funding from the Centre Hospitalier Universitaire de Bordeaux. ZX has research grant funding from the National Institute of Neurological Disorders and Stroke (NINDS). None of these funding sources had any role in supporting the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication. All the other authors have no conflicts of interests to declare.
Figures
References
-
- Lambrou A.S., Shirk P., Steele M.K., et al. Morbidity and mortality weekly report genomic surveillance for SARS-CoV-2 variants: predominance of the delta (B.1.617.2) and Omicron (B.1.1.529) variants-United States. Morb Mortal Wkly Rep. 2022;71(6):206–211. https://www.cdc.gov/mmwr/volumes/71/wr/mm7106a4.htm#F1_down - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
